

Cervical cancer screening using HPV tests on self-samples: attitudes and preferences of women participating in the VALHUDES study
- PMID: 34462004
- PMCID: PMC8403820
- DOI: 10.1186/s13690-021-00667-4
Cervical cancer screening using HPV tests on self-samples: attitudes and preferences of women participating in the VALHUDES study
Abstract
Background: Interventions to reach women who do not participate regularly in screening may reduce the risk of cervical cancer. Self-collection of a vaginal specimen has been shown to increase participation. The relative clinical accuracy of human papillomavirus (HPV) testing on first-void urine (with Colli-Pee) and on vaginal self-samples versus on cervical clinician-collected samples is being investigated in the VALHUDES trial. The current study assesses attitudes and experiences regarding self-sampling among women enrolled in VALHUDES.
Methods: Questionnaires from 515 women (age 25-64 years [N = 498]; < 25 [N = 10], age ≥ 65 [N = 3], enrolled between December 2017 - January 2020) referred to colposcopy because of previous cervical abnormalities and enrolled in VALHUDES (NCT03064087) were analysed.
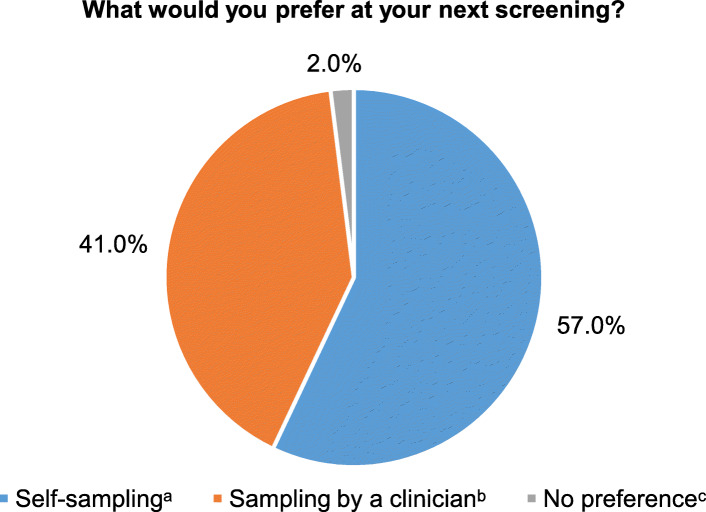
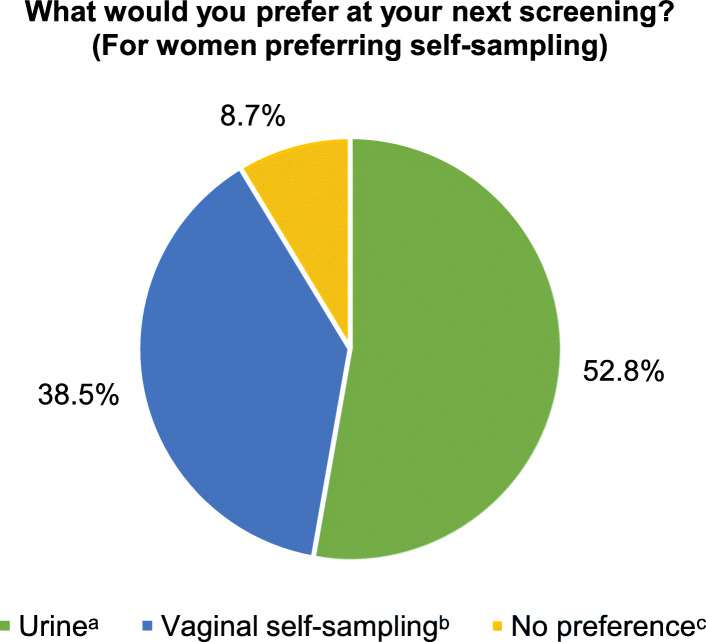
Results: Of the 515 participants, nearly all women confirmed that self-sampling may help in reaching under-screened women (93%). Nevertheless, 44% of the participants stated before starting collection that a clinician-collected sample is more effective than a self-collected sample. After self-sampling, the large majority of women (> 95%) declared that instructions for self-collection were clear, that collection was easy, and that they were confident about having performed the procedure correctly, for both urine and vaginal collection. However, a proportion of women found self-sampling unpleasant (9.5% [49/515] for urine collection; 18.6% [96/515] and 15.5% [80/515] for vaginal sampling with cotton swabs or plastic brushes, respectively). For their next screening round, 57% would prefer self-sampling whereas 41% opted for collection by a clinician. Among women preferring self-sampling, 53% would choose for urine collection, 38% for vaginal self-collection and 9% had no preference. Age did not modify preferences.
Conclusion: We conclude that both urine and vaginal self-sampling are well accepted by women, with a preference for urine sampling. Although the large majority of women are confident in their ability to perform self-sampling, four to five over ten women preferred specimen collection by a clinician.
Trial registration: The study VALHUDES was registered in ClinicalTrials.gov (identifier: NCT03064087 ).
Keywords: Attitudes; Cervical cancer; HPV; Human papillomavirus; Preferences; Screening; Self-sampling; Urine; VALHUDES.
© 2021. The Author(s).
Conflict of interest statement
H De Pauw, E Peeters and M Arbyn are supported by the RISCC Network funded by the Horizon 2020 Framework of DG Research and Innovation, European Commission, Brussels, Belgium (grant No. 847845). S Van Keer is supported by a junior postdoctoral fellowship of the Research Foundation – Flanders (FWO), Belgium (Grant Number: 1240220 N). A Vorsters is co-founder of Novosanis (Belgium), a spin-off company of the University of Antwerp, and was minority shareholder until January 2019. D Vanden Broeck is employed by AML, a commercial lab performing cervical cytology and HPV testing. All other authors declare no personal conflicts of interest.
Figures
Similar articles
-
Clinical Performance of the RealTime High Risk HPV Assay on Self-Collected Vaginal Samples within the VALHUDES Framework.Microbiol Spectr. 2022 Oct 26;10(5):e0163122. doi: 10.1128/spectrum.01631-22. Epub 2022 Sep 1. Microbiol Spectr. 2022. PMID: 36047900 Free PMC article.
-
Home-based urinary HPV self-sampling for the detection of cervical cancer precursor lesions: attitudes and preferences from Belgian females participating in the CASUS study.Arch Public Health. 2025 Feb 12;83(1):32. doi: 10.1186/s13690-024-01490-3. Arch Public Health. 2025. PMID: 39934916 Free PMC article.
-
Validation of BD Onclarity HPV Assay on Vaginal Self-Samples versus Cervical Samples Using the VALHUDES Protocol.Cancer Epidemiol Biomarkers Prev. 2022 Dec 5;31(12):2177-2184. doi: 10.1158/1055-9965.EPI-22-0757. Cancer Epidemiol Biomarkers Prev. 2022. PMID: 36099441
-
Self-Sampling for Human Papillomavirus Testing: Increased Cervical Cancer Screening Participation and Incorporation in International Screening Programs.Front Public Health. 2018 Apr 9;6:77. doi: 10.3389/fpubh.2018.00077. eCollection 2018. Front Public Health. 2018. PMID: 29686981 Free PMC article. Review.
-
Accuracy analysis of cervical cancer screening using urine and vaginal self-sampling versus clinician-collected samples: A systematic review and meta-analysis.Int J Gynaecol Obstet. 2025 May 13. doi: 10.1002/ijgo.70207. Online ahead of print. Int J Gynaecol Obstet. 2025. PMID: 40357572 Review.
Cited by
-
Self-sampling as the principal modality for population based cervical screening: Five-year follow-up of the PaVDaG study.Int J Cancer. 2022 Apr 15;150(8):1350-1356. doi: 10.1002/ijc.33888. Epub 2021 Dec 6. Int J Cancer. 2022. PMID: 34850395 Free PMC article.
-
Attitude toward human papillomavirus self-sampling and associated factors among Thai women undergoing colposcopy.Obstet Gynecol Sci. 2024 May;67(3):286-295. doi: 10.5468/ogs.23293. Epub 2024 Mar 8. Obstet Gynecol Sci. 2024. PMID: 38454573 Free PMC article.
-
Testing for Human Papillomaviruses in Urine, Blood, and Oral Specimens: an Update for the Laboratory.J Clin Microbiol. 2023 Aug 23;61(8):e0140322. doi: 10.1128/jcm.01403-22. Epub 2023 Jul 13. J Clin Microbiol. 2023. PMID: 37439692 Free PMC article. Review.
-
Attitudes towards being offered a choice of self-sampling or clinician sampling for cervical screening: A cross-sectional survey of women taking part in a clinical validation of HPV self-collection devices.J Med Screen. 2025 Jun;32(2):93-99. doi: 10.1177/09691413241283356. Epub 2024 Oct 9. J Med Screen. 2025. PMID: 39383889 Free PMC article.
-
Utilizing first void urine for high-risk HPV testing for cervical cancer screening in HIV-positive women in Katete, Zambia.BMC Womens Health. 2023 Feb 11;23(1):62. doi: 10.1186/s12905-023-02212-7. BMC Womens Health. 2023. PMID: 36774526 Free PMC article.
References
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
