

Dual PD-L1 and TGF-b blockade in patients with recurrent respiratory papillomatosis
- PMID: 34462327
- PMCID: PMC8407210
- DOI: 10.1136/jitc-2021-003113
Dual PD-L1 and TGF-b blockade in patients with recurrent respiratory papillomatosis
Erratum in
-
Correction: Dual PD-L1 and TGF-b blockade in patients with recurrent respiratory papillomatosis.J Immunother Cancer. 2021 Oct;9(10):1. doi: 10.1136/jitc-2021-003113corr1. J Immunother Cancer. 2021. PMID: 34663642 Free PMC article. No abstract available.
Abstract
Background: Recurrent respiratory papillomatosis (RRP) is a human papillomavirus (HPV) driven neoplastic disorder of the upper aerodigestive tract that causes significant morbidity and can lead to fatal airway obstruction. Prior clinical study demonstrated clinical benefit with the programmed death-ligand 1 (PD-L1) monoclonal antibody avelumab. Bintrafusp alpha is a bifunctional inhibitor of PD-L1 and transforming growth factor-beta (TGF-b) that has shown clinical activity in several cancer types.
Methods: We conducted a phase II clinical trial evaluating bintrafusp alpha in adults with RRP. Papilloma samples before and after treatment with bintrafusp alpha were assessed for correlates of response with multiplex immunofluorescence as well as immunological and genomic analyses. Post hoc analyses of papilloma samples before and after treatment with avelumab were assessed for comparison.
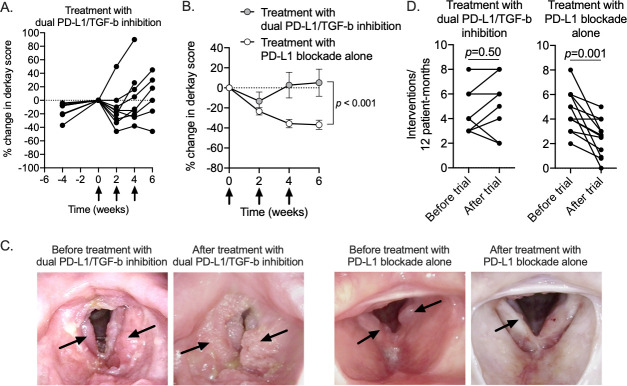
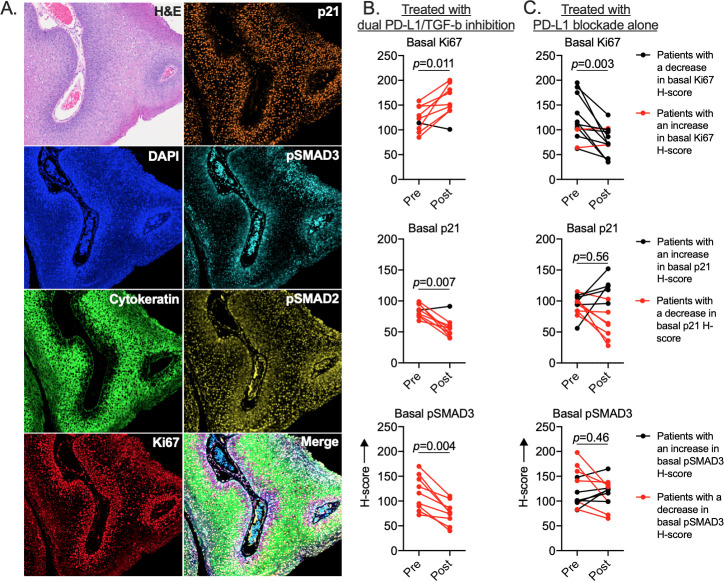
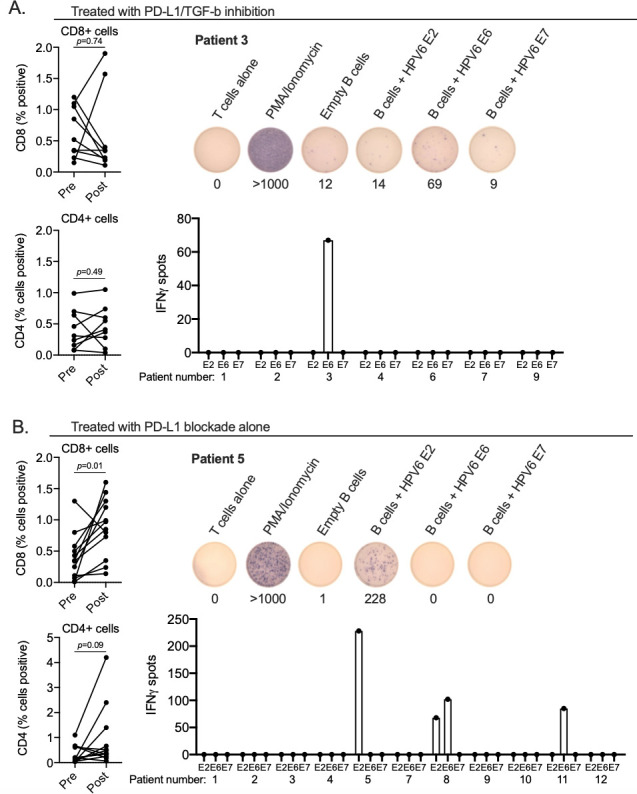
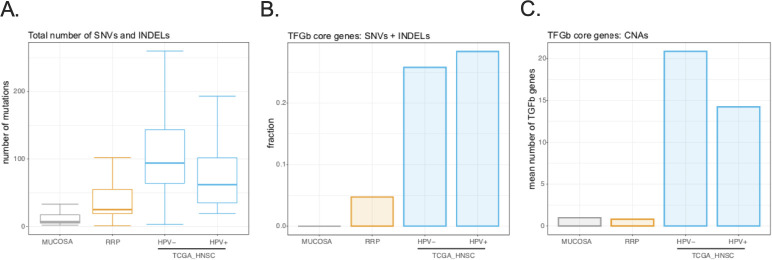
Results: Dual PD-L1/TGF-b inhibition failed to abrogate papilloma growth in most subjects and increased the frequency of clinically indicated interventions after treatment in four of eight subjects based on each subject's own historical control. TGF-b neutralization consistently decreased pSMAD3 and p21 and increased Ki67 expression within the basal layers of papillomas, indicating that TGF-b restrained proliferation. These alterations were not observed in papillomas treated with PD-L1 blockade alone. Dual PD-L1/TGF-b inhibition did not enhance anti-HPV immunity within papillomas beyond that observed with PD-L1 blockade. Genomic alterations in TGF-b superfamily genes were infrequent in papillomas and normal mucosa but present in a significant fraction of head and neck carcinomas.
Conclusions: Intact TGF-b signaling restrains proliferation within papillomas, and the use of clinical agents that abrogate this pathway should be avoided in patients with RRP.
Trial registration numbers: NCT03707587 and NCT02859454.
Keywords: head and neck neoplasms; immunohistochemistry; immunotherapy; investigational; therapies; tumor microenvironment.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None.
Figures
References
Publication types
MeSH terms
Substances
Supplementary concepts
Associated data
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials