

Functional data analysis characterizes the shapes of the first COVID-19 epidemic wave in Italy
- PMID: 34462450
- PMCID: PMC8405612
- DOI: 10.1038/s41598-021-95866-y
Functional data analysis characterizes the shapes of the first COVID-19 epidemic wave in Italy
Abstract
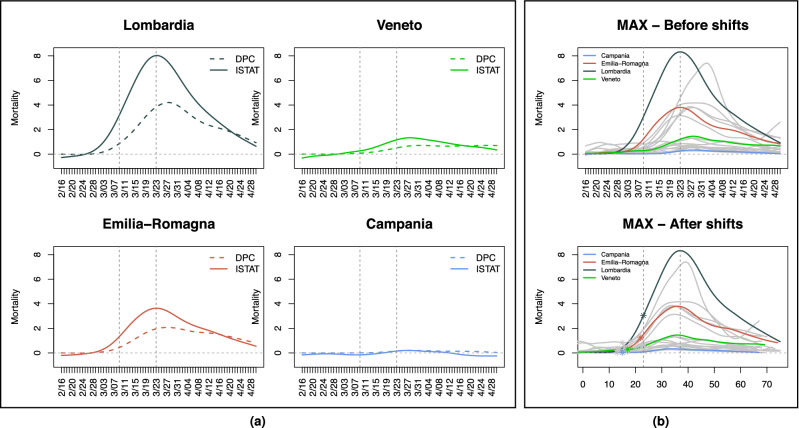
We investigate patterns of COVID-19 mortality across 20 Italian regions and their association with mobility, positivity, and socio-demographic, infrastructural and environmental covariates. Notwithstanding limitations in accuracy and resolution of the data available from public sources, we pinpoint significant trends exploiting information in curves and shapes with Functional Data Analysis techniques. These depict two starkly different epidemics; an "exponential" one unfolding in Lombardia and the worst hit areas of the north, and a milder, "flat(tened)" one in the rest of the country-including Veneto, where cases appeared concurrently with Lombardia but aggressive testing was implemented early on. We find that mobility and positivity can predict COVID-19 mortality, also when controlling for relevant covariates. Among the latter, primary care appears to mitigate mortality, and contacts in hospitals, schools and workplaces to aggravate it. The techniques we describe could capture additional and potentially sharper signals if applied to richer data.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures





References
-
- ISTAT. Demographic indicators. http://dati.istat.it/Index.aspx?DataSetCode=DCIS_INDDEMOG1&Lang=en.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
