

Campylobacter jejuni genotypes are associated with post-infection irritable bowel syndrome in humans
- PMID: 34462533
- PMCID: PMC8405632
- DOI: 10.1038/s42003-021-02554-8
Campylobacter jejuni genotypes are associated with post-infection irritable bowel syndrome in humans
Abstract
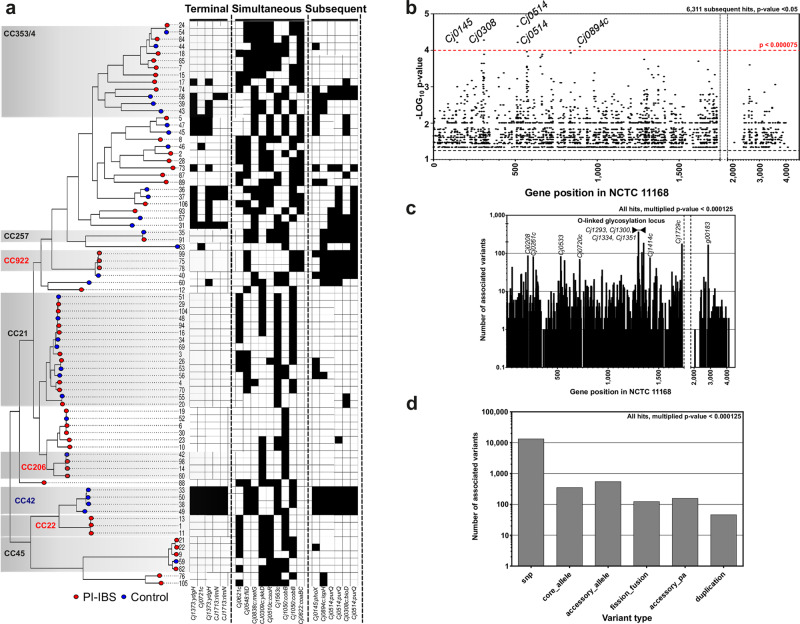
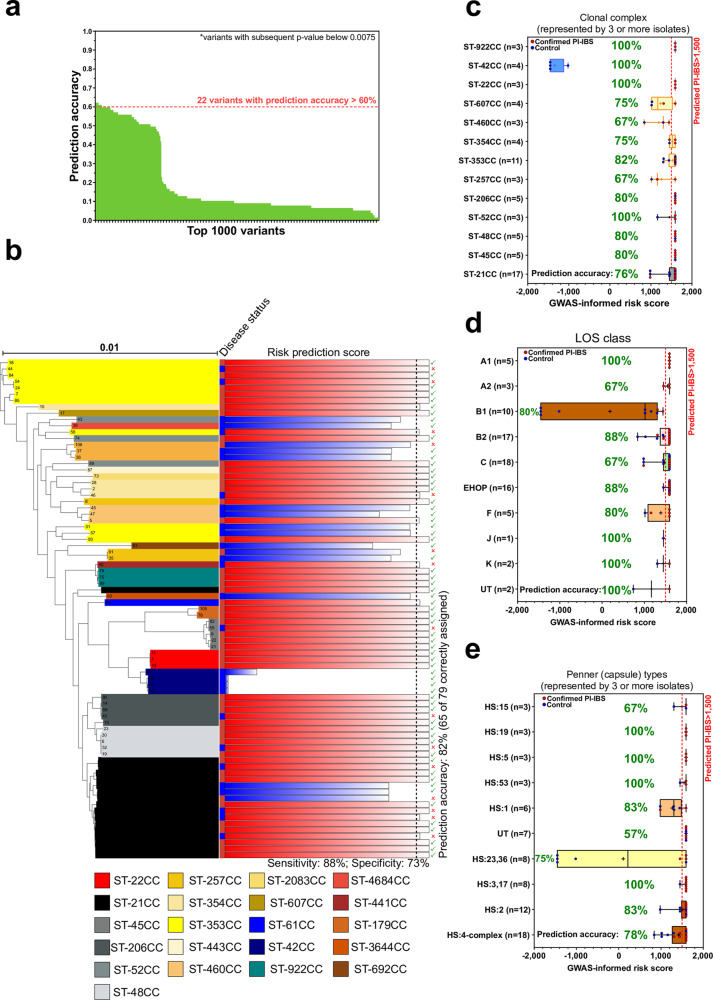
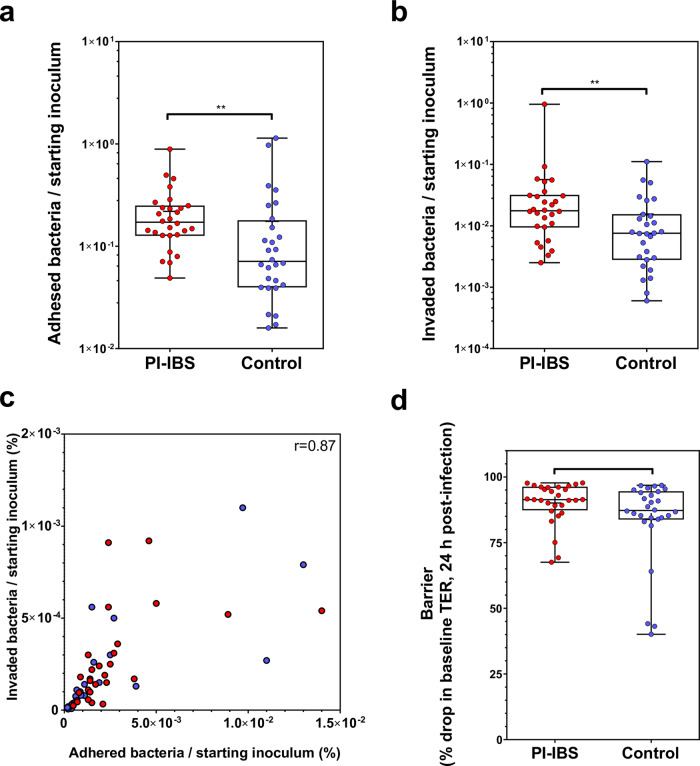
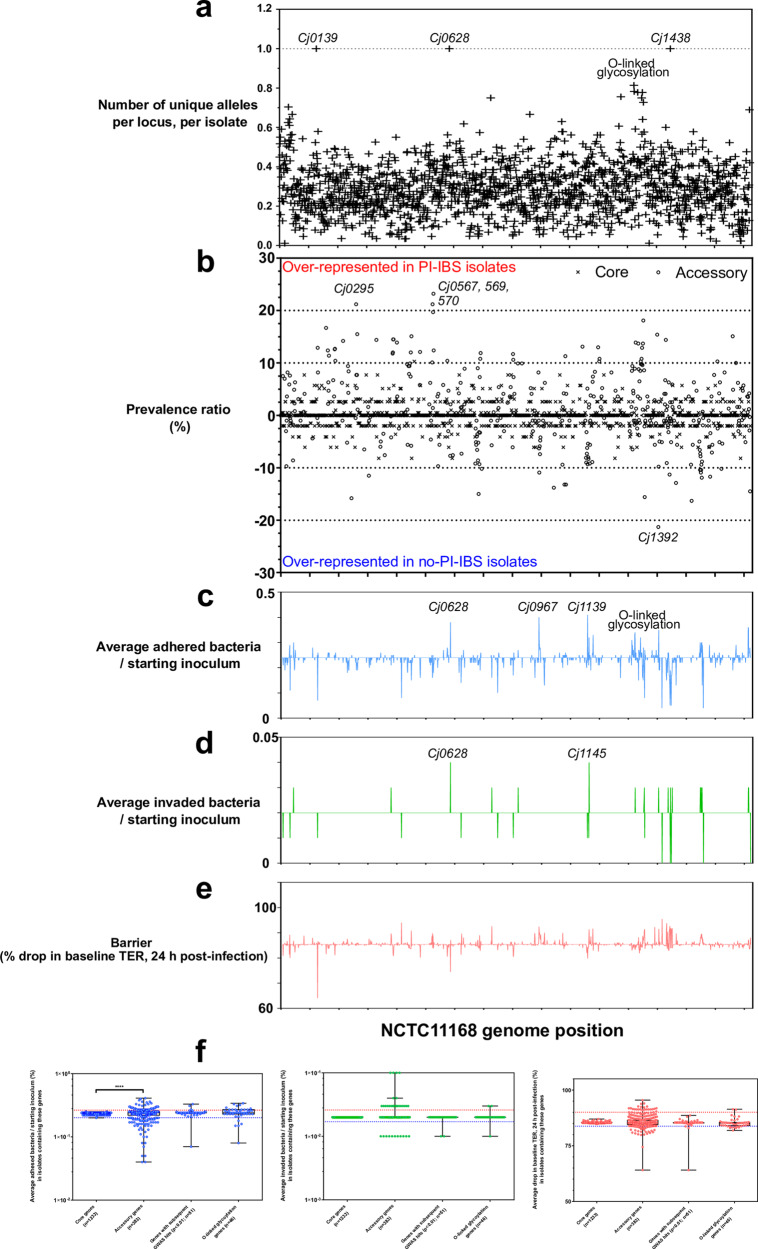
Campylobacter enterocolitis may lead to post-infection irritable bowel syndrome (PI-IBS) and while some C. jejuni strains are more likely than others to cause human disease, genomic and virulence characteristics promoting PI-IBS development remain uncharacterized. We combined pangenome-wide association studies and phenotypic assays to compare C. jejuni isolates from patients who developed PI-IBS with those who did not. We show that variation in bacterial stress response (Cj0145_phoX), adhesion protein (Cj0628_CapA), and core biosynthetic pathway genes (biotin: Cj0308_bioD; purine: Cj0514_purQ; isoprenoid: Cj0894c_ispH) were associated with PI-IBS development. In vitro assays demonstrated greater adhesion, invasion, IL-8 and TNFα secretion on colonocytes with PI-IBS compared to PI-no-IBS strains. A risk-score for PI-IBS development was generated using 22 genomic markers, four of which were from Cj1631c, a putative heme oxidase gene linked to virulence. Our finding that specific Campylobacter genotypes confer greater in vitro virulence and increased risk of PI-IBS has potential to improve understanding of the complex host-pathogen interactions underlying this condition.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Mearin, F. et al. Bowel disorders. Gastroenterology10.1053/j.gastro.2016.02.031 (2016).
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
