

This is a preprint.
Immune responses in COVID-19 respiratory tract and blood reveal mechanisms of disease severity
- PMID: 34462740
- PMCID: PMC8404907
- DOI: 10.21203/rs.3.rs-802084/v1
Immune responses in COVID-19 respiratory tract and blood reveal mechanisms of disease severity
Update in
-
SARS-CoV-2 infection results in immune responses in the respiratory tract and peripheral blood that suggest mechanisms of disease severity.Nat Commun. 2022 May 19;13(1):2774. doi: 10.1038/s41467-022-30088-y. Nat Commun. 2022. PMID: 35589689 Free PMC article.
Abstract
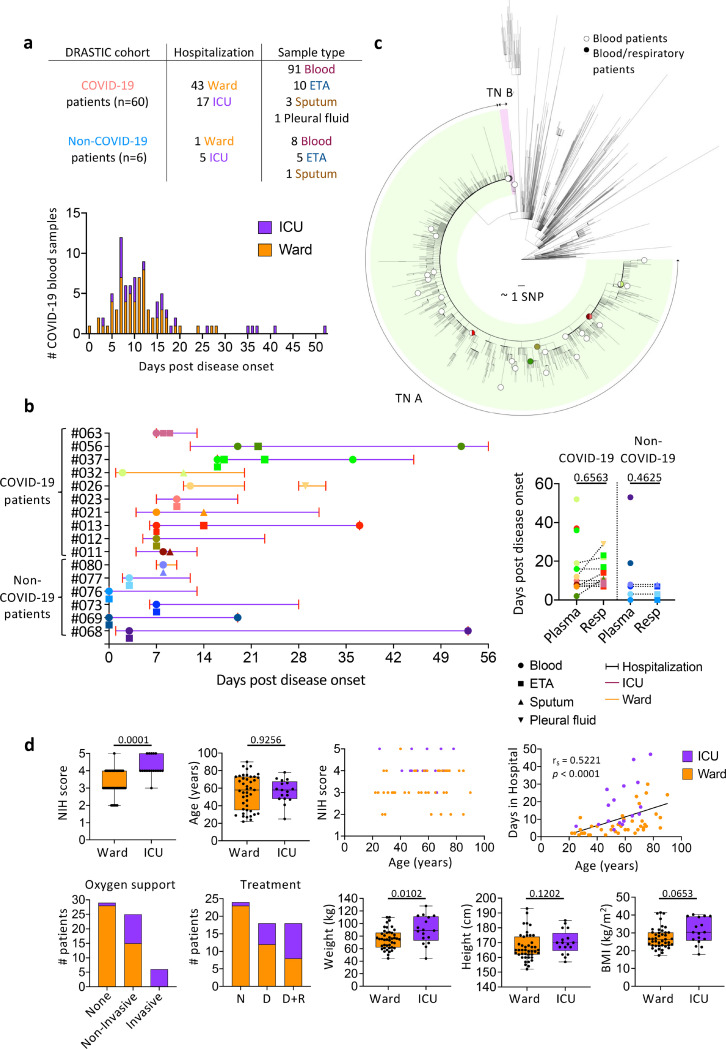
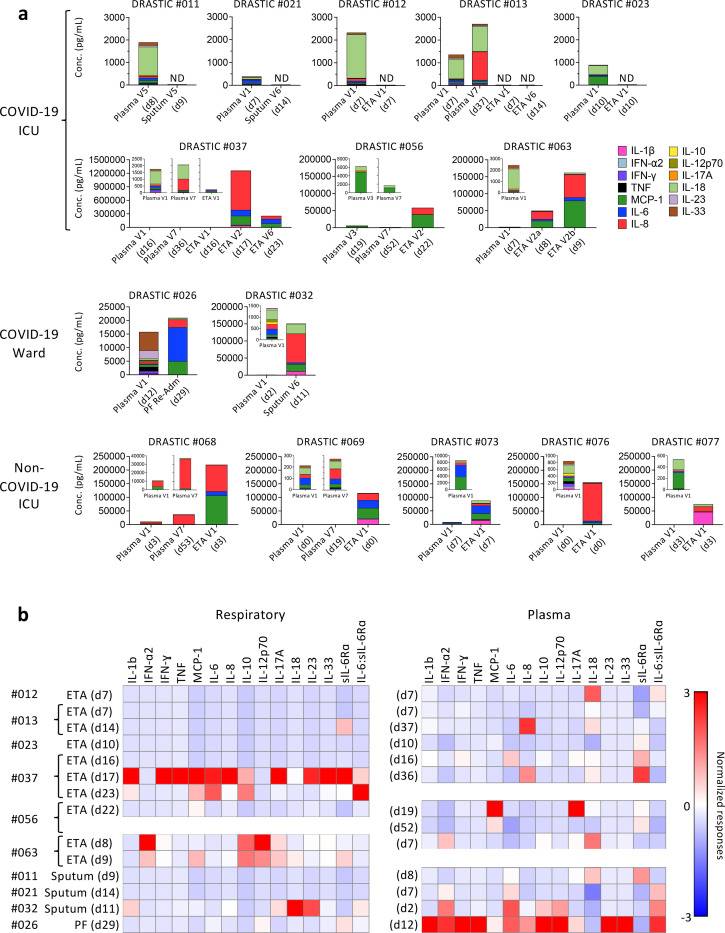
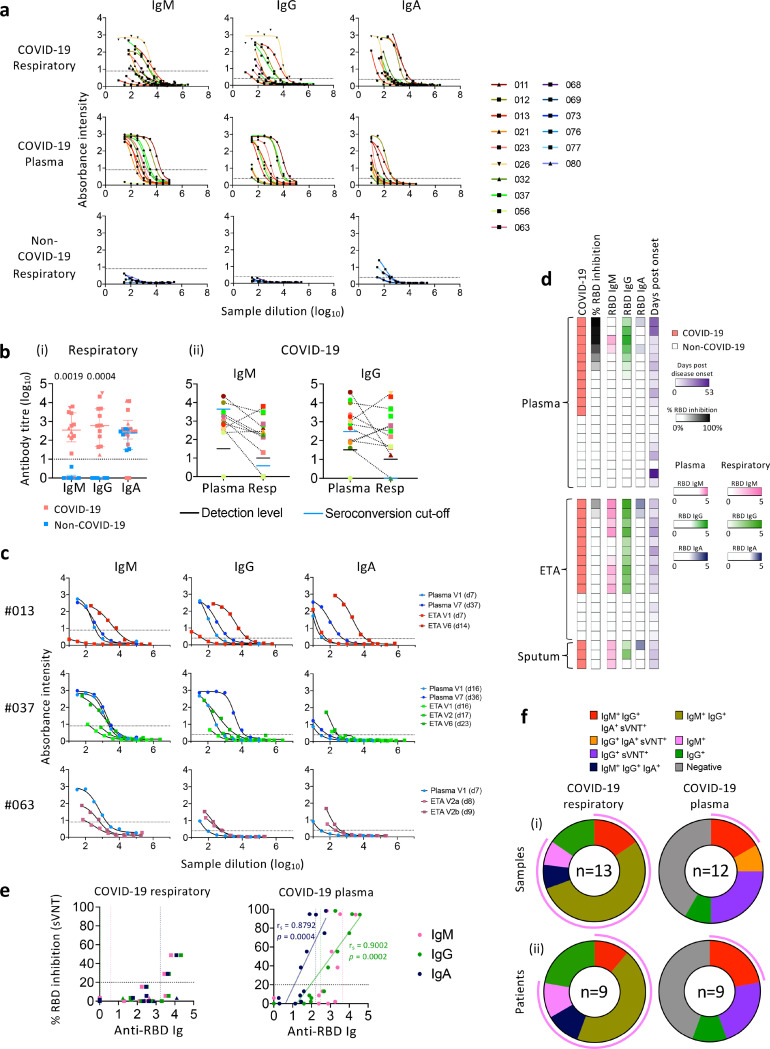
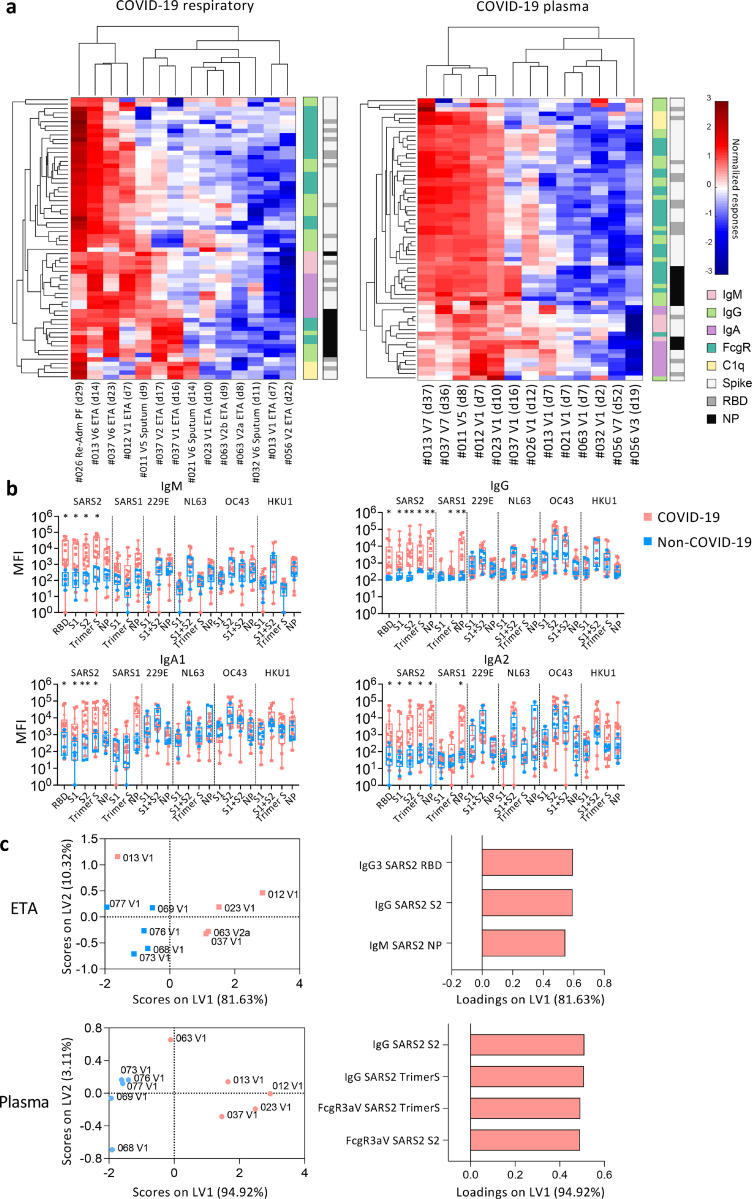
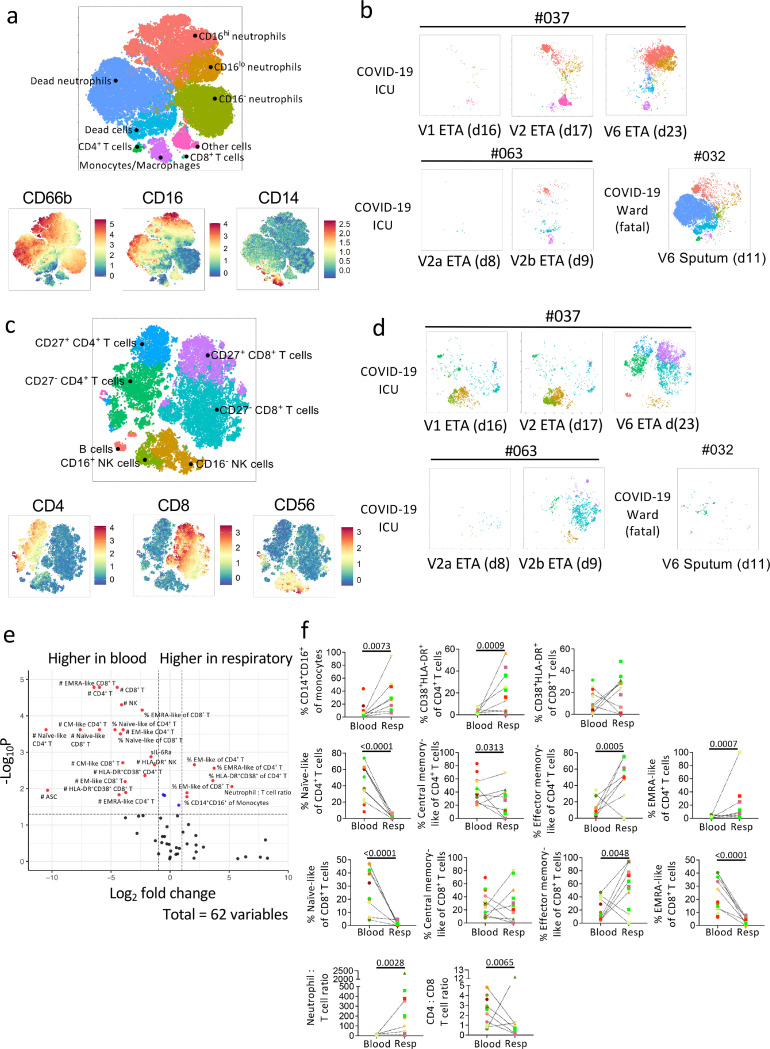
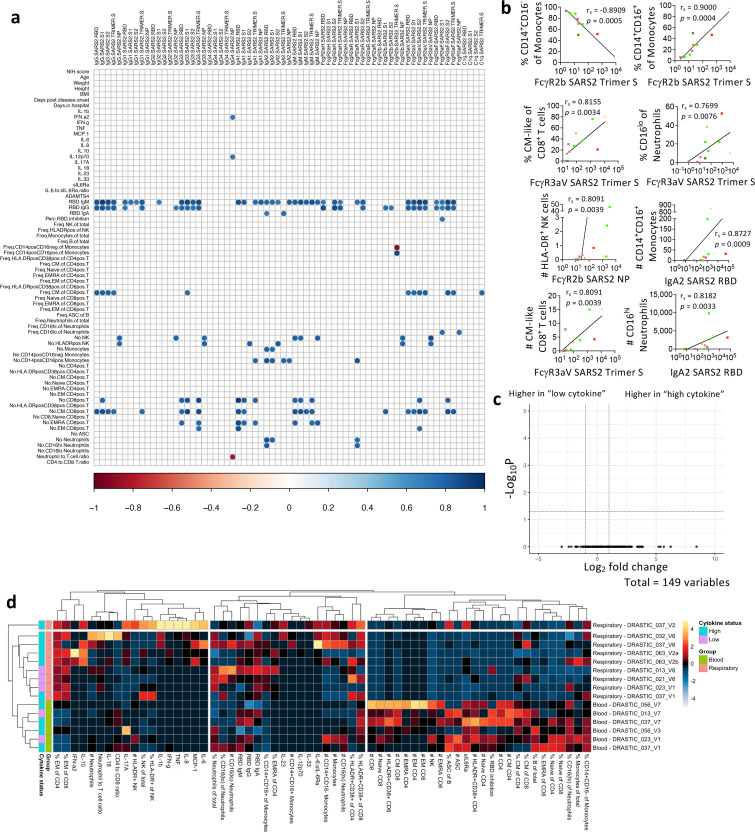
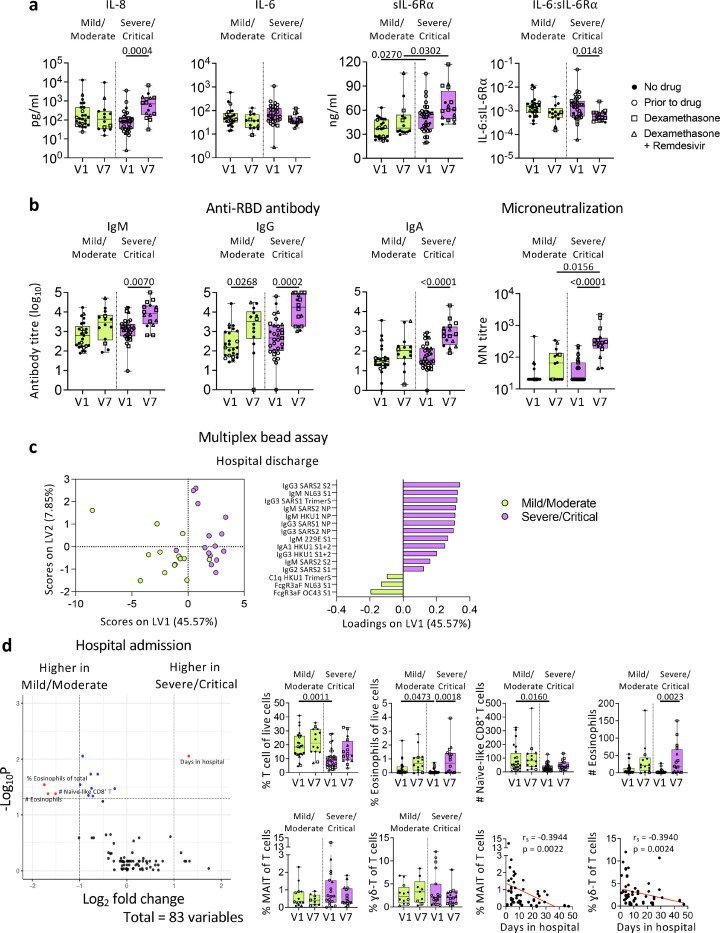
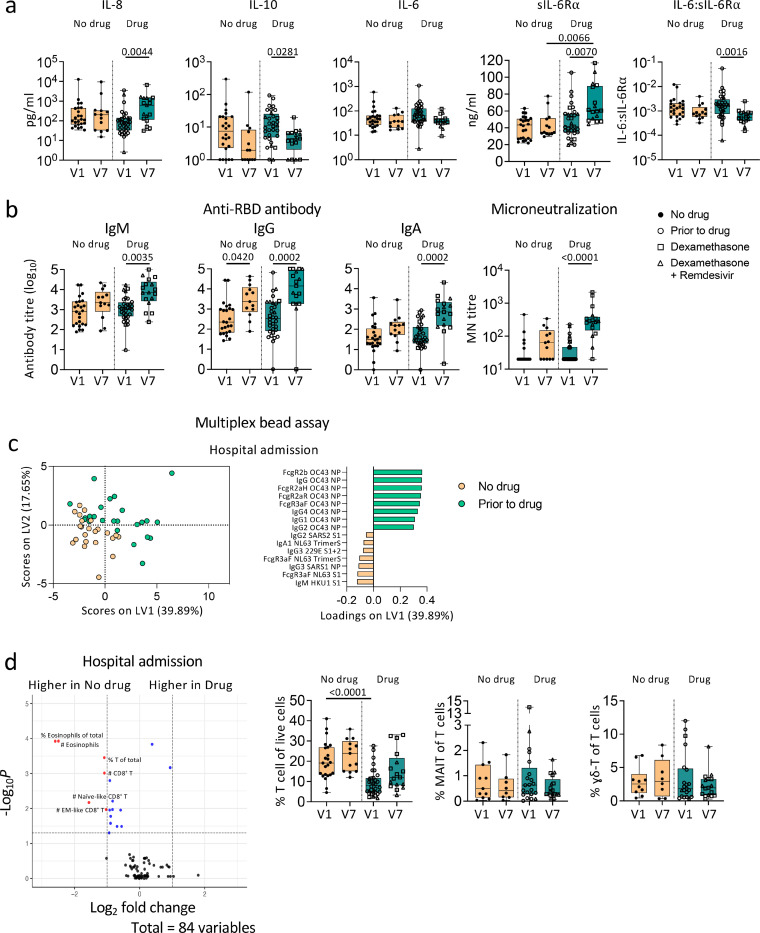
Although the respiratory tract is the primary site of SARS-CoV-2 infection and the ensuing immunopathology, respiratory immune responses are understudied and urgently needed to understand mechanisms underlying COVID-19 disease pathogenesis. We collected paired longitudinal blood and respiratory tract samples (endotracheal aspirate, sputum or pleural fluid) from hospitalized COVID-19 patients and non-COVID-19 controls. Cellular, humoral and cytokine responses were analysed and correlated with clinical data. SARS-CoV-2-specific IgM, IgG and IgA antibodies were detected using ELISA and multiplex assay in both the respiratory tract and blood of COVID-19 patients, although a higher receptor binding domain (RBD)-specific IgM and IgG seroconversion level was found in respiratory specimens. SARS-CoV-2 neutralization activity in respiratory samples was detected only when high levels of RBD-specific antibodies were present. Strikingly, cytokine/chemokine levels and profiles greatly differed between respiratory samples and plasma, indicating that inflammation needs to be assessed in respiratory specimens for the accurate assessment of SARS-CoV-2 immunopathology. Diverse immune cell subsets were detected in respiratory samples, albeit dominated by neutrophils. Importantly, we also showed that dexamethasone and/or remdesivir treatment did not affect humoral responses in blood of COVID-19 patients. Overall, our study unveils stark differences in innate and adaptive immune responses between respiratory samples and blood and provides important insights into effect of drug therapy on immune responses in COVID-19 patients.
Conflict of interest statement
Declaration of Interests
The authors declare no competing interests.
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
