

This is a preprint.
Profiling Transcription Initiation in Peripheral Leukocytes Reveals Severity-Associated Cis-Regulatory Elements in Critical COVID-19
- PMID: 34462742
- PMCID: PMC8404884
- DOI: 10.1101/2021.08.24.457187
Profiling Transcription Initiation in Peripheral Leukocytes Reveals Severity-Associated Cis-Regulatory Elements in Critical COVID-19
Update in
-
Dynamic activity in cis-regulatory elements of leukocytes identifies transcription factor activation and stratifies COVID-19 severity in ICU patients.Cell Rep Med. 2023 Feb 21;4(2):100935. doi: 10.1016/j.xcrm.2023.100935. Epub 2023 Jan 25. Cell Rep Med. 2023. PMID: 36758547 Free PMC article.
Abstract
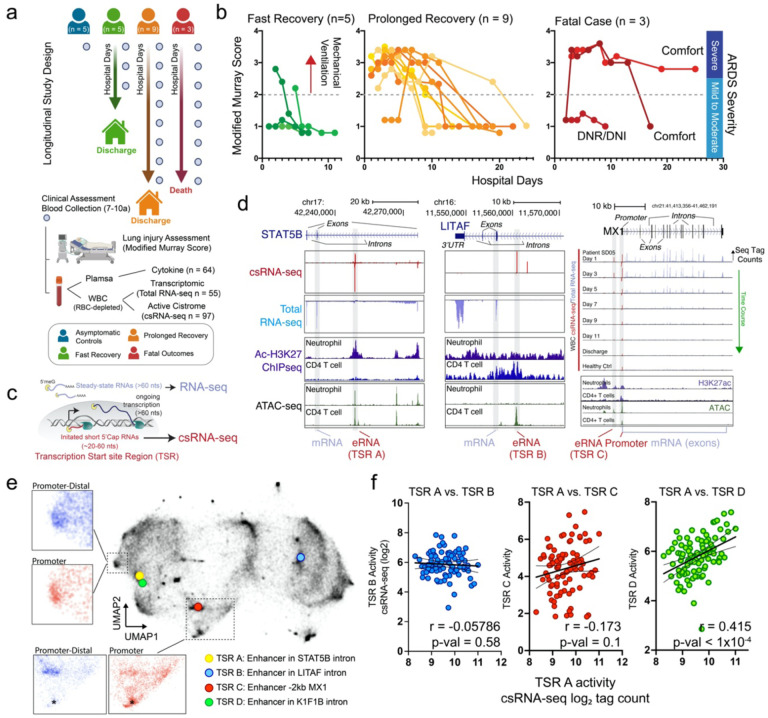
The contribution of transcription factors (TFs) and gene regulatory programs in the immune response to COVID-19 and their relationship to disease outcome is not fully understood. Analysis of genome-wide changes in transcription at both promoter-proximal and distal cis-regulatory DNA elements, collectively termed the 'active cistrome,' offers an unbiased assessment of TF activity identifying key pathways regulated in homeostasis or disease. Here, we profiled the active cistrome from peripheral leukocytes of critically ill COVID-19 patients to identify major regulatory programs and their dynamics during SARS-CoV-2 associated acute respiratory distress syndrome (ARDS). We identified TF motifs that track the severity of COVID- 19 lung injury, disease resolution, and outcome. We used unbiased clustering to reveal distinct cistrome subsets delineating the regulation of pathways, cell types, and the combinatorial activity of TFs. We found critical roles for regulatory networks driven by stimulus and lineage determining TFs, showing that STAT and E2F/MYB regulatory programs targeting myeloid cells are activated in patients with poor disease outcomes and associated with single nucleotide genetic variants implicated in COVID-19 susceptibility. Integration with single-cell RNA-seq found that STAT and E2F/MYB activation converged in specific neutrophils subset found in patients with severe disease. Collectively we demonstrate that cistrome analysis facilitates insight into disease mechanisms and provides an unbiased approach to evaluate global changes in transcription factor activity and stratify patient disease severity.
Figures





References
-
- Liao M, Liu Y, Yuan J, Wen Y, Xu G, Zhao J, et al. Single-cell landscape of bronchoalveolar immune cells in patients with COVID-19. Nature medicine. 2020;26(6):842–4. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous