

High unbound flucloxacillin fraction in critically ill patients
- PMID: 34463730
- PMCID: PMC8598283
- DOI: 10.1093/jac/dkab314
High unbound flucloxacillin fraction in critically ill patients
Abstract
Objectives: To describe the unbound and total flucloxacillin pharmacokinetics in critically ill patients and to define optimal dosing strategies.
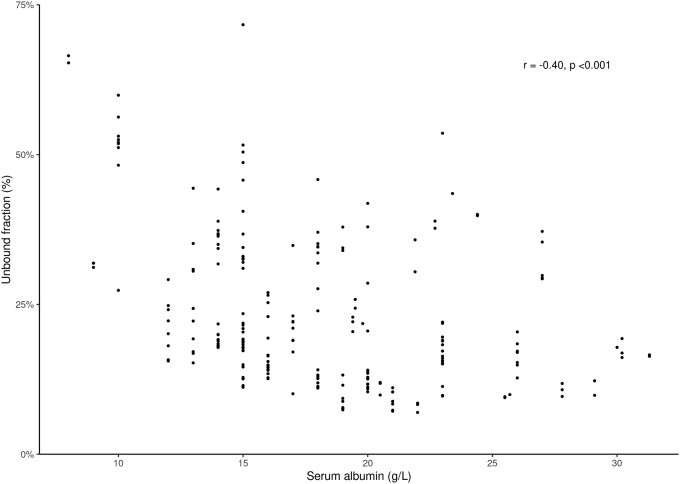
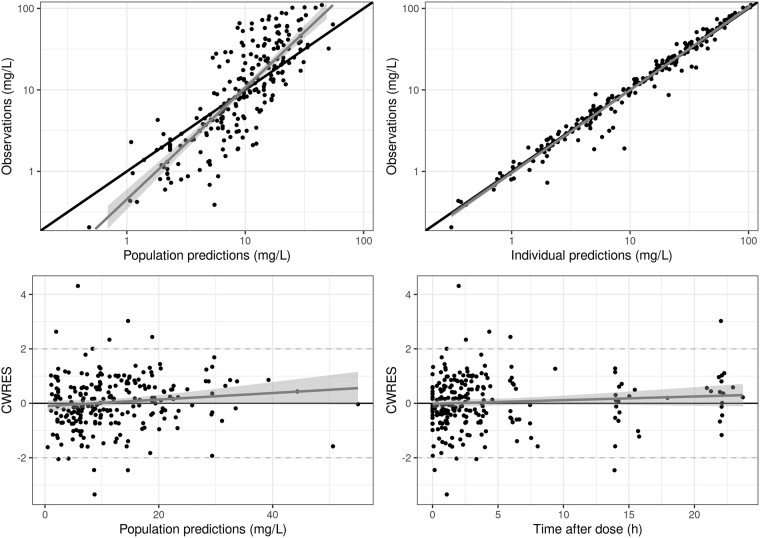
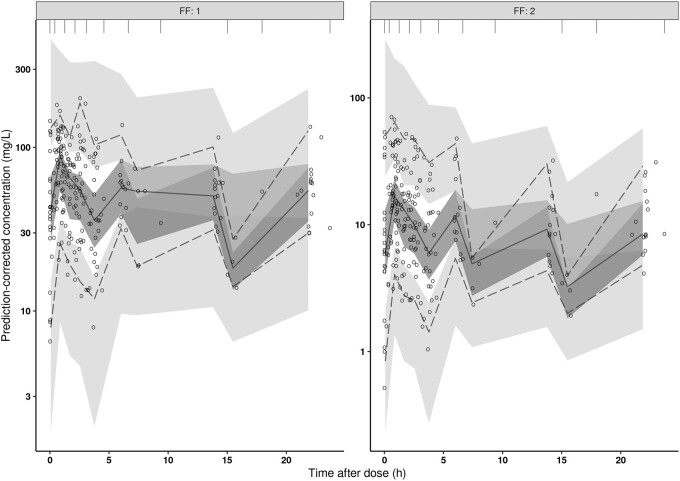
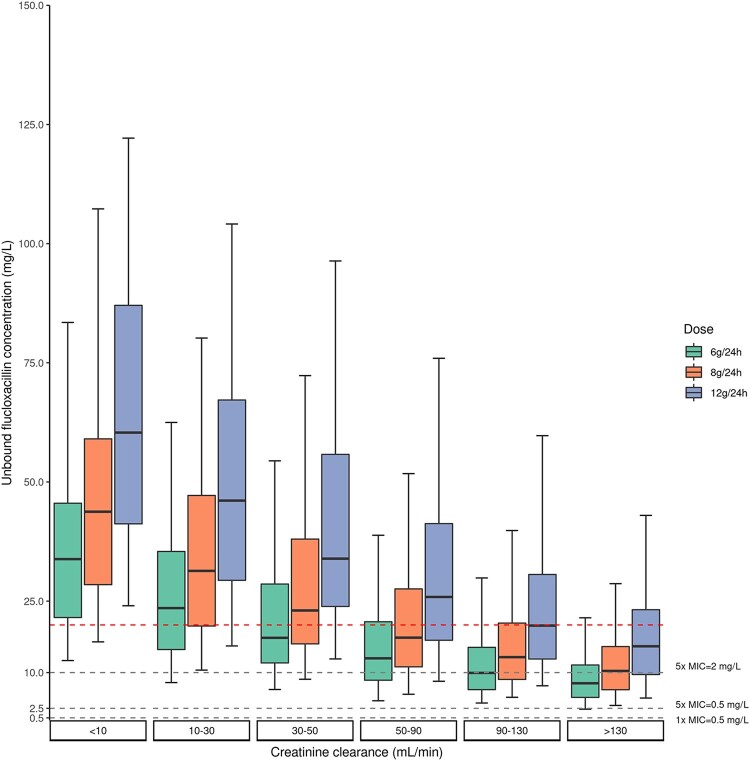
Patients and methods: Observational multicentre study including a total of 33 adult ICU patients receiving flucloxacillin, given as intermittent or continuous infusion. Pharmacokinetic sampling was performed on two occasions on two different days. Total and unbound flucloxacillin concentrations were measured and analysed using non-linear mixed-effects modelling. Serum albumin was added as covariate on the maximum binding capacity and endogenous creatinine clearance (CLCR) as covariate for renal function. Monte Carlo simulations were performed to predict the unbound flucloxacillin concentrations for different dosing strategies and different categories of endogenous CLCR.
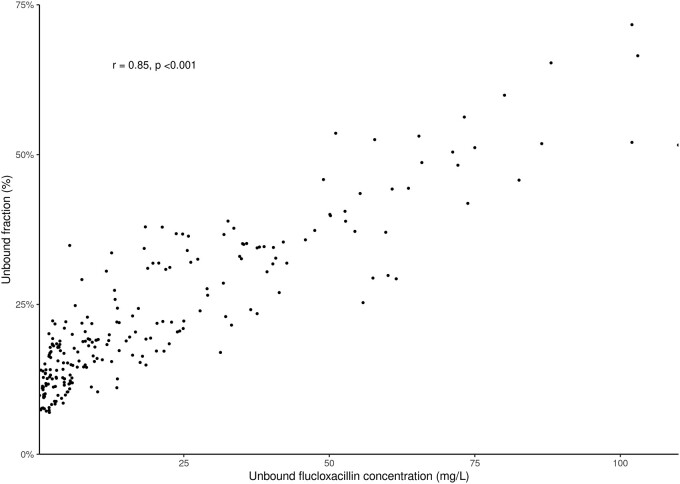
Results: The measured unbound concentrations ranged from 0.2 to 110 mg/L and the observed unbound fraction varied between 7.0% and 71.7%. An integral two-compartmental linear pharmacokinetic model based on total and unbound concentrations was developed. A dose of 12 g/24 h was sufficient for 99.9% of the population to achieve a concentration of >2.5 mg/L (100% fT>5×MIC, MIC = 0.5 mg/L).
Conclusions: Critically ill patients show higher unbound flucloxacillin fractions and concentrations than previously thought. Consequently, the risk of subtherapeutic exposure is low.
© The Author(s) 2021. Published by Oxford University Press on behalf of the British Society for Antimicrobial Chemotherapy.
Figures
References
-
- Summary of product characteristics Floxapen®, poeder voor oplossing voor injectie 250 mg, 500 mg en 1 g. 2021. https://www.geneesmiddeleninformatiebank.nl/smpc/h05990_smpc.pdf.
-
- Rijnders MI, Deurenberg RH, Boumans ML. et al. Flucloxacillin, still the empirical choice for putative Staphylococcus aureus infections in intensive care units in the Netherlands. J Antimicrob Chemother 2009; 64: 1029–34. - PubMed
-
- Ulldemolins M, Roberts JA, Wallis SC. et al. Flucloxacillin dosing in critically ill patients with hypoalbuminaemia: special emphasis on unbound pharmacokinetics. J Antimicrob Chemother 2010; 65: 1771–8. - PubMed
