

Integrated Biomarkers for the Management of Indeterminate Pulmonary Nodules
- PMID: 34464235
- PMCID: PMC8786067
- DOI: 10.1164/rccm.202012-4438OC
Integrated Biomarkers for the Management of Indeterminate Pulmonary Nodules
Abstract
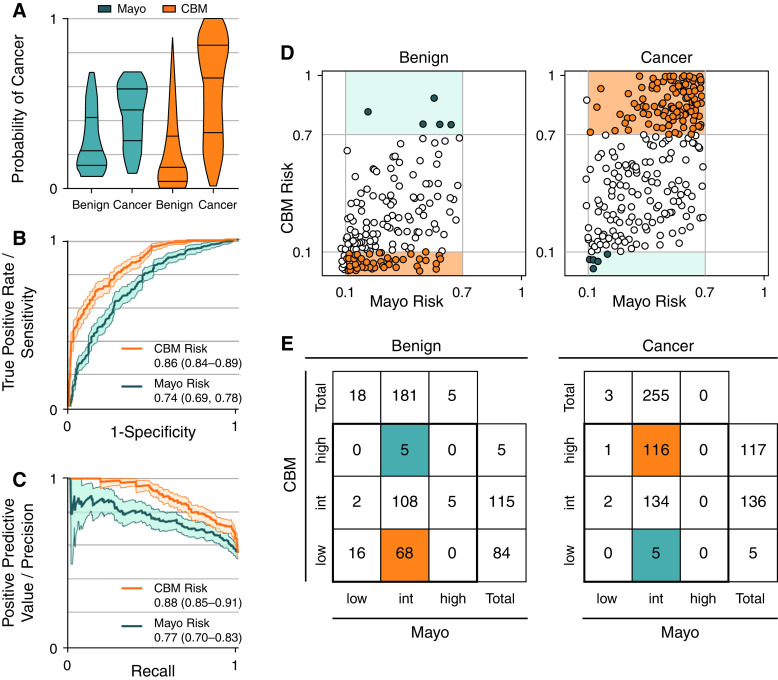
Rationale: Patients with indeterminate pulmonary nodules (IPNs) at risk of cancer undergo high rates of invasive, costly, and morbid procedures. Objectives: To train and externally validate a risk prediction model that combined clinical, blood, and imaging biomarkers to improve the noninvasive management of IPNs. Methods: In this prospectively collected, retrospective blinded evaluation study, probability of cancer was calculated for 456 patient nodules using the Mayo Clinic model, and patients were categorized into low-, intermediate-, and high-risk groups. A combined biomarker model (CBM) including clinical variables, serum high sensitivity CYFRA 21-1 level, and a radiomic signature was trained in cohort 1 (n = 170) and validated in cohorts 2-4 (total n = 286). All patients were pooled to recalibrate the model for clinical implementation. The clinical utility of the CBM compared with current clinical care was evaluated in 2 cohorts. Measurements and Main Results: The CBM provided improved diagnostic accuracy over the Mayo Clinic model with an improvement in area under the curve of 0.124 (95% bootstrap confidence interval, 0.091-0.156; P < 2 × 10-16). Applying 10% and 70% risk thresholds resulted in a bias-corrected clinical reclassification index for cases and control subjects of 0.15 and 0.12, respectively. A clinical utility analysis of patient medical records estimated that a CBM-guided strategy would have reduced invasive procedures from 62.9% to 50.6% in the intermediate-risk benign population and shortened the median time to diagnosis of cancer from 60 to 21 days in intermediate-risk cancers. Conclusions: Integration of clinical, blood, and image biomarkers improves noninvasive diagnosis of patients with IPNs, potentially reducing the rate of unnecessary invasive procedures while shortening the time to diagnosis.
Keywords: biomarkers; diagnostic imaging; lung neoplasms; tumor.
Figures

Comment in
-
Integrated Biomarkers for Pulmonary Nodules: Proving What Is Possible.Am J Respir Crit Care Med. 2021 Dec 1;204(11):1247-1248. doi: 10.1164/rccm.202108-2002ED. Am J Respir Crit Care Med. 2021. PMID: 34582716 Free PMC article. No abstract available.
-
Reply to Zhao et al.: Integrated Biomarkers for Indeterminate Pulmonary Nodules: Is 2-Year Imaging Follow-Up Enough for Suspected Benign Lesions?Am J Respir Crit Care Med. 2022 Jun 15;205(12):1486. doi: 10.1164/rccm.202201-0082LE. Am J Respir Crit Care Med. 2022. PMID: 35373716 Free PMC article. No abstract available.
-
Integrated Biomarkers for Indeterminate Pulmonary Nodules: Is 2-Year Imaging Follow-Up Enough for Suspected Benign Lesions?Am J Respir Crit Care Med. 2022 Jun 15;205(12):1485-1486. doi: 10.1164/rccm.202111-2648LE. Am J Respir Crit Care Med. 2022. PMID: 35373720 Free PMC article. No abstract available.
References
-
- Gould MK, Tang T, Liu I-LA, Lee J, Zheng C, Danforth KN, et al. Recent trends in the identification of incidental pulmonary nodules. Am J Respir Crit Care Med . 2015;192:1208–1214. - PubMed
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin . 2018;68:7–30. - PubMed
-
- Lokhandwala T, Bittoni MA, Dann RA, D’Souza AO, Johnson M, Nagy RJ, et al. Costs of diagnostic assessment for lung cancer: a Medicare claims analysis. Clin Lung Cancer . 2017;18:e27–e34. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
