

Diagnostic performance and clinical implications of rapid SARS-CoV-2 antigen testing in Mexico using real-world nationwide COVID-19 registry data
- PMID: 34464393
- PMCID: PMC8407542
- DOI: 10.1371/journal.pone.0256447
Diagnostic performance and clinical implications of rapid SARS-CoV-2 antigen testing in Mexico using real-world nationwide COVID-19 registry data
Abstract
Background: SARS-CoV-2 testing capacity is important to monitor epidemic dynamics and as a mitigation strategy. Given difficulties of large-scale quantitative reverse transcription polymerase chain reaction (qRT-PCR) implementation, rapid antigen tests (Rapid Ag-T) have been proposed as alternatives in settings like Mexico. Here, we evaluated diagnostic performance of Rapid Ag-T for SARS-CoV-2 infection and its associated clinical implications compared to qRT-PCR testing in Mexico.
Methods: We analyzed data from the COVID-19 registry of the Mexican General Directorate of Epidemiology up to April 30th, 2021 (n = 6,632,938) and cases with both qRT-PCR and Rapid Ag-T (n = 216,388). We evaluated diagnostic performance using accuracy measures and assessed time-dependent changes in the Area Under the Receiver Operating Characteristic curve (AUROC). We also explored test discordances as predictors of hospitalization, intubation, severe COVID-19 and mortality.
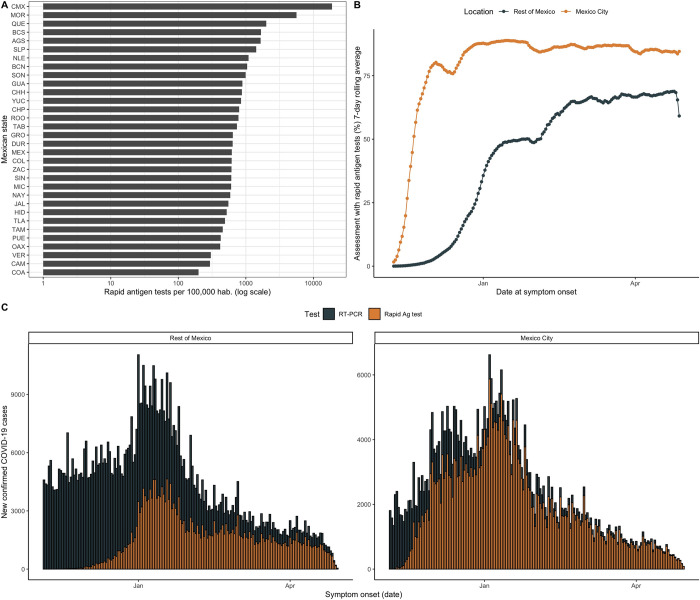
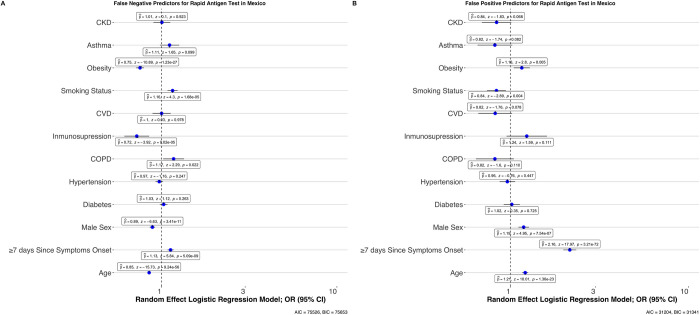
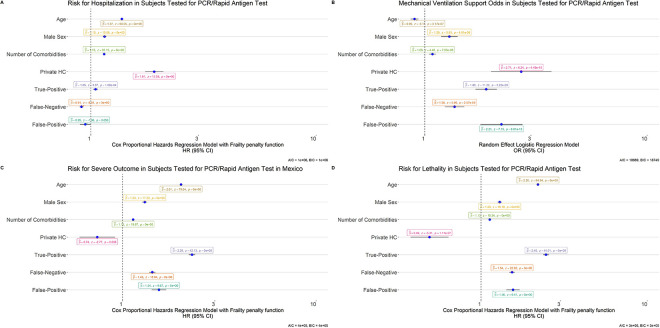
Results: Rapid Ag-T is primarily used in Mexico City. Rapid Ag-T have low sensitivity 37.6% (95%CI 36.6-38.7), high specificity 95.5% (95%CI 95.1-95.8) and acceptable positive 86.1% (95%CI 85.0-86.6) and negative predictive values 67.2% (95%CI 66.2-69.2). Rapid Ag-T has optimal diagnostic performance up to days 3 after symptom onset, and its performance is modified by testing location, comorbidity, and age. qRT-PCR (-) / Rapid Ag-T (+) cases had higher risk of adverse COVID-19 outcomes (HR 1.54 95% CI 1.41-1.68) and were older, qRT-PCR (+)/ Rapid Ag-T(-) cases had slightly higher risk or adverse outcomes and ≥7 days from symptom onset (HR 1.53 95% CI 1.48-1.59). Cases detected with rapid Ag-T were younger, without comorbidities, and milder COVID-19 course.
Conclusions: Rapid Ag-T could be used as an alternative to qRT-PCR for large scale SARS-CoV-2 testing in Mexico. Interpretation of Rapid Ag-T results should be done with caution to minimize the risk associated with false negative results.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Tracking COVID-19: Contact Tracing in the Digital Age. Accessed January 2, 2021. https://www.who.int/news-room/feature-stories/detail/tracking-covid-19-c...
-
- WHO Emergency Use Listing for In vitro diagnostics (IVDs) Detecting SARS-CoV-2. Accessed January 1, 2021. https://www.who.int/publications/m/item/200922-eul-sars-cov2-product-list
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
