

Anaesthetic depth and delirium after major surgery: a randomised clinical trial
- PMID: 34465469
- PMCID: PMC8579421
- DOI: 10.1016/j.bja.2021.07.021
Anaesthetic depth and delirium after major surgery: a randomised clinical trial
Abstract
Background: Postoperative delirium is a serious complication of surgery associated with prolonged hospitalisation, long-term cognitive decline, and mortality. This study aimed to determine whether targeting bispectral index (BIS) readings of 50 (light anaesthesia) was associated with a lower incidence of POD than targeting BIS readings of 35 (deep anaesthesia).
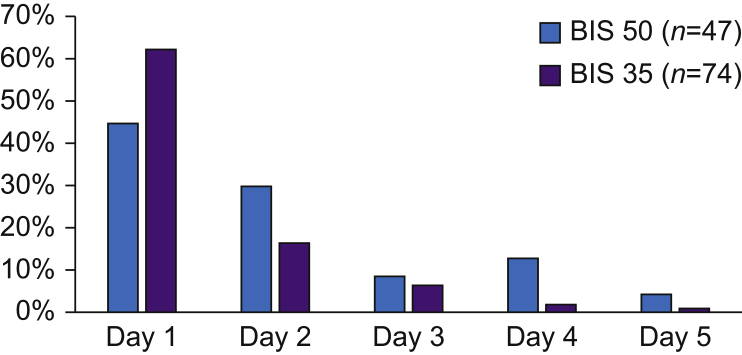
Methods: This multicentre randomised clinical trial of 655 at-risk patients undergoing major surgery from eight centres in three countries assessed delirium for 5 days postoperatively using the 3 min confusion assessment method (3D-CAM) or CAM-ICU, and cognitive screening using the Mini-Mental State Examination at baseline and discharge and the Abbreviated Mental Test score (AMTS) at 30 days and 1 yr. Patients were assigned to light or deep anaesthesia. The primary outcome was the presence of postoperative delirium on any of the first 5 postoperative days. Secondary outcomes included mortality at 1 yr, cognitive decline at discharge, cognitive impairment at 30 days and 1 yr, unplanned ICU admission, length of stay, and time in electroencephalographic burst suppression.
Results: The incidence of postoperative delirium in the BIS 50 group was 19% and in the BIS 35 group was 28% (odds ratio 0.58 [95% confidence interval: 0.38-0.88]; P=0.010). At 1 yr, those in the BIS 50 group demonstrated significantly better cognitive function than those in the BIS 35 group (9% with AMTS ≤6 vs 20%; P<0.001).
Conclusions: Among patients undergoing major surgery, targeting light anaesthesia reduced the risk of postoperative delirium and cognitive impairment at 1 yr.
Clinical trial registration: ACTRN12612000632897.
Keywords: anaesthesia; bispectral index; cognitive dysfunction; delirium; electroencephalography; postoperative delirium.
Copyright © 2021 British Journal of Anaesthesia. Published by Elsevier Ltd. All rights reserved.
Figures

Comment in
-
Anaesthetic depth and delirium: a challenging balancing act.Br J Anaesth. 2021 Nov;127(5):667-671. doi: 10.1016/j.bja.2021.08.003. Epub 2021 Sep 6. Br J Anaesth. 2021. PMID: 34503835
-
The quagmire of postoperative delirium: does dose matter?Br J Anaesth. 2021 Nov;127(5):664-666. doi: 10.1016/j.bja.2021.08.008. Epub 2021 Sep 8. Br J Anaesth. 2021. PMID: 34507823 No abstract available.
-
Beware the drug titration paradox. Comment on Br J Anaesth 2021; 127: 704-12.Br J Anaesth. 2022 Jun;128(6):e335-e337. doi: 10.1016/j.bja.2022.01.004. Epub 2022 Feb 4. Br J Anaesth. 2022. PMID: 35131097 No abstract available.
-
How balanced is the BALANCED delirium trial? Comment on Br J Anaesth 2021; 127: 704-12.Br J Anaesth. 2022 Apr;128(4):e274-e275. doi: 10.1016/j.bja.2022.01.018. Epub 2022 Feb 17. Br J Anaesth. 2022. PMID: 35183347 No abstract available.
-
Anaesthetic depth and delirium after major surgery. Comment on Br J Anaesth 2022; 127: 704-12.Br J Anaesth. 2022 Aug;129(2):e33-e35. doi: 10.1016/j.bja.2022.05.001. Epub 2022 May 30. Br J Anaesth. 2022. PMID: 35654630 No abstract available.
References
-
- Silbert B.S., Scott D.A., Evered L.A., et al. A comparison of the effect of high- and low-dose fentanyl on the incidence of postoperative cognitive dysfunction after coronary artery bypass surgery in the elderly. Anesthesiology. 2006;104:1137–1145. - PubMed
-
- Evered L.A., Silbert B.S., Scott D.A., Maruff P., Ames D. Prevalence of dementia 7.5 years after coronary artery bypass graft surgery. Anesthesiology. 2016;125:62–71. - PubMed
-
- O’Regan N.A., Fitzgerald J., Timmons S., O’Connell H., Meagher D. Delirium: a key challenge for perioperative care. Int J Surg. 2013;11:136–144. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
