

CD4+ T cell and M2 macrophage infiltration predict dedifferentiated liposarcoma patient outcomes
- PMID: 34465597
- PMCID: PMC8413967
- DOI: 10.1136/jitc-2021-002812
CD4+ T cell and M2 macrophage infiltration predict dedifferentiated liposarcoma patient outcomes
Abstract
Background: Dedifferentiated liposarcoma (DDLPS) is one of the most common soft tissue sarcoma subtypes and is devastating in the advanced/metastatic stage. Despite the observation of clinical responses to PD-1 inhibitors, little is known about the immune microenvironment in relation to patient prognosis.
Methods: We performed a retrospective study of 61 patients with DDLPS. We completed deep sequencing of the T-cell receptor (TCR) β-chain and RNA sequencing for predictive modeling, evaluating both immune markers and tumor escape genes. Hierarchical clustering and recursive partitioning were employed to elucidate relationships of cellular infiltrates within the tumor microenvironment, while an immune score for single markers was created as a predictive tool.
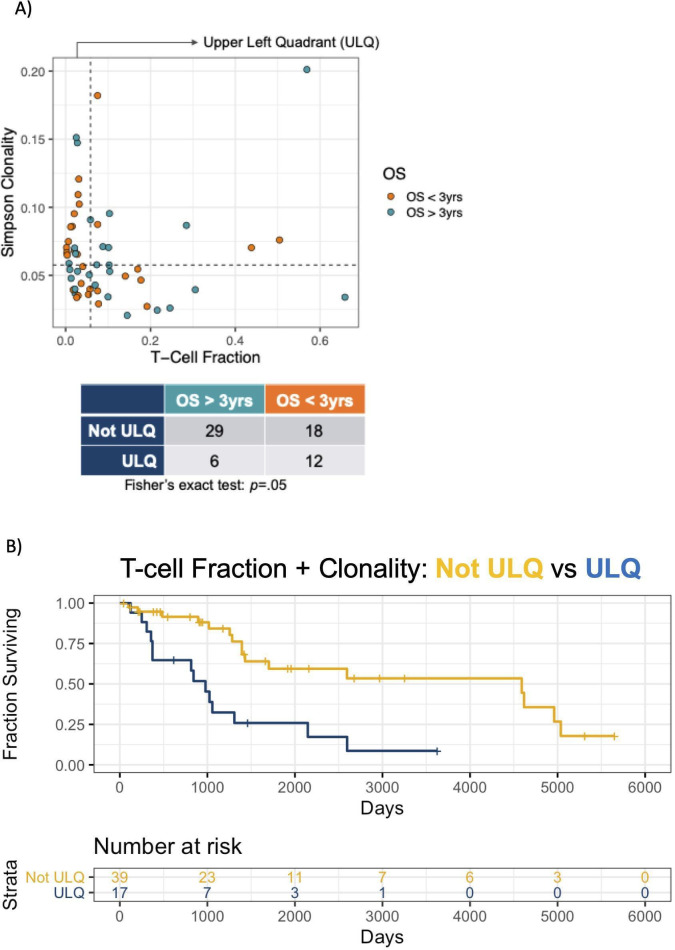
Results: Although many DDLPS samples had low TCR clonality, high TCR clonality combined with low T-cell fraction predicted lower 3-year overall survival (p=0.05). Higher levels of CD14+ monocytes (p=0.02) inversely correlated with 3-year recurrence-free survival (RFS), while CD4+ T-cell infiltration (p=0.05) was associated with a higher RFS. Genes associated with longer RFS included PD-1 (p=0.003), ICOS (p=0.006), BTLA (p=0.033), and CTLA4 (p=0.02). In a composite immune score, CD4+ T cells had the strongest positive predictive value, while CD14+ monocytes and M2 macrophages had the strongest negative predictive values.
Conclusions: Immune cell infiltration predicts clinical outcome in DDLPS, with CD4+ cells associated with better outcomes; CD14+ cells and M2 macrophages are associated with worse outcomes. Future checkpoint inhibitor studies in DDLPS should incorporate immunosequencing and gene expression profiling techniques that can generate immune landscape profiles.
Keywords: CD4-positive T-lymphocytes; immunity; macrophages; sarcoma; tumor microenvironment.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: BAS, SZ, LRS, BCS, KSS, JGM, EC, JSC, and RHP declare no potential conflicts of interest. SMP reported research funding from Merck during the conduct of the study; research funding from EMD Serono, Incyte, Presage, Janssen, OncoSec, and Juno and consulting, honoraria, and advisory activity with GlaxoSmithKline, Eli Lilly and Company, Seattle Genetics, Bayer, Tempus, Daiichi Sankyo, and Blueprint Medicine, outside the submitted work. NAL and KCF are employed by Cofactor Genomics, Inc, the company that developed and produces the ImmunoPrism® reagent kit and informatics tools used in this article. BJL is a paid consultant for Cofactor Genomics, Inc. RMG and MV have a financial interest in Adaptive Biotechnologies. JR has equity in Adaptive Biotechnologies, equity and employment with Bristol Myers Squibb. MJW reported research funding from Athenex, Deciphera, Incyte, Tempus, Adaptimmune, and GlaxoSmithKline and consulting, honoraria, and advisory activity with Tempus, Deciphera, and Adaptimmune, outside the submitted work. RLJ reported grants from Merck during the conduct of the study; research support from Merck Sharp & Dohme and GlaxoSmithKline and consultation fees from Adaptimmune, Athenex, Blueprint Medicine, Clinigen, Eisai, Epizyme, Daiichi Sankyo, Deciphera, Immune Design, Eli Lilly and Company, Merck, Pharma Mar, and UpToDate, outside the submitted work; in addition, RLJ had a patent to biomarker, issued. LDC receives research funding, paid to institution, from Eli Lilly, AADi, BluePrint Medicine, Iterion, Gradalis, Philogen, Advenchen Laboratories, and CBA Pharma. LDC institution has received funding from Eli Lilly for conduct of clinical trials. LDC has received honoraria or has served on advisory boards for BluePrint Medicines and Regeneron.
Figures




References
-
- Demetri GD, von Mehren M, Jones RL, et al. Efficacy and safety of trabectedin or dacarbazine for metastatic liposarcoma or leiomyosarcoma after failure of conventional chemotherapy: results of a phase III randomized multicenter clinical trial. JCO 2016;34:786–93. 10.1200/JCO.2015.62.4734 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials