

Automated versus manual urine output monitoring in the intensive care unit
- PMID: 34465821
- PMCID: PMC8408210
- DOI: 10.1038/s41598-021-97026-8
Automated versus manual urine output monitoring in the intensive care unit
Abstract
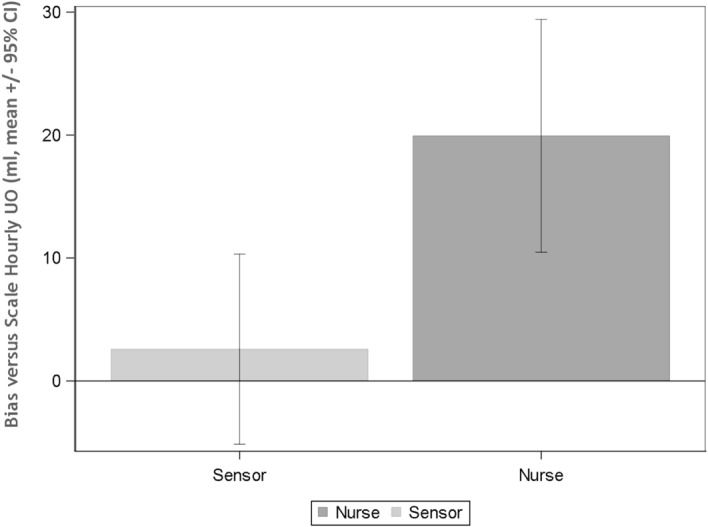
Acute kidney injury (AKI) is defined by changes in serum creatinine and urine output (UO). Significant limitations exist regarding accurate ascertainment of urine output even within the intensive care unit. We sought to evaluate an automated urine output collections system and compare it to nursing measurements. We prospectively collected urine output using an electronic urine monitoring system and compared it to charted hourly UO in 44 patients after cardiac surgery at a single university hospital ICU. We calculated UO and oliguria rates and compared them to data from the sensor and from nursing charting. A total of 187 hourly UO measurements were obtained and on average, UO was reported 47 min late, with a median of 18 min, and a maximum of almost 6 h. Patients had a mean hourly UO of 76.3 ml over the observation period. Compared to manual measurements by study personnel, nurses significantly overestimated hourly UO by 19.9 ml (95% CI: 10.3; 29.5; p = < 0.001). By contrast, the mean difference between the UO measured with the sensor and by study personnel was 2.29 ml (95% CI: - 6.7; 11.3), p = 0.61. Electronic UO monitoring is significantly more accurate than nurse-performed manual measurements in actual intensive care patients. Furthermore, timely ascertainment of UO is difficult to achieve with manual technique, resulting in important delays in detecting oliguria perhaps leading to missed cases of AKI.
© 2021. The Author(s).
Conflict of interest statement
JAK reports consulting fees from RenalSense. No other authors report any competing interests.
Figures
References
-
- Priyanka P, Zarbock A, Izawa J, Gleason TG, Renfurm RW, Kellum JA. The impact of acute kidney injury by serum creatinine or urine output criteria on major adverse kidney events in cardiac surgery patients. J. Thorac Cardiovasc. Surg. 2020;162:143–151. doi: 10.1016/j.jtcvs.2019.11.137. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
