

Venetoclax-resistant CLL cells show a highly activated and proliferative phenotype
- PMID: 34467417
- PMCID: PMC10992976
- DOI: 10.1007/s00262-021-03043-x
Venetoclax-resistant CLL cells show a highly activated and proliferative phenotype
Abstract
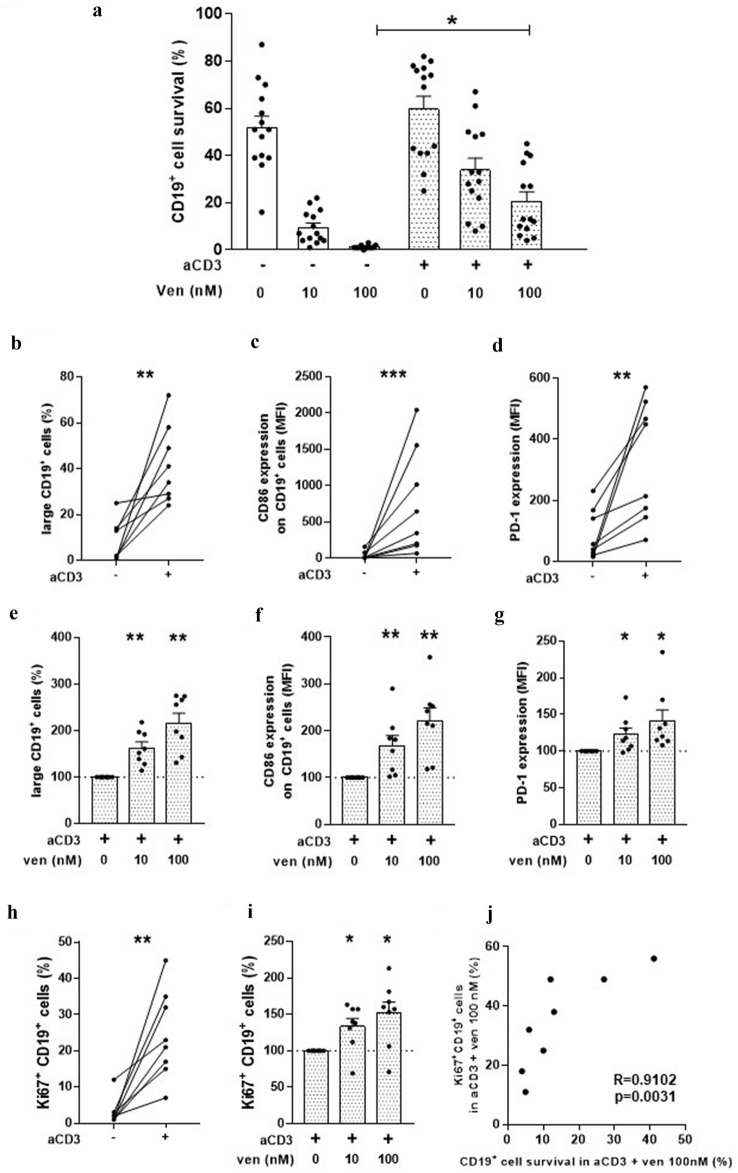
Venetoclax treatment has demonstrated efficacy and a safety profile in chronic lymphocytic leukemia (CLL) patients, however the emergence of resistant cells is a current complication. We and others, previously reported that the activation of CLL cells by signals that mimic microenvironment stimuli favors the upregulation of anti-apoptotic proteins from B cell lymphoma-2 (BCL-2) family that are not targeted by venetoclax, reducing malignant cell sensitivity to the drug. We here studied venetoclax-resistant CLL cells generated in vitro by autologous activated T lymphocytes, and found that they showed an aggressive phenotype characterized by increased expression of activation and proliferation markers. Moreover, surviving cells expressed high levels of B cell lymphoma-extra-large (BCL-XL) and/or myeloid cell leukemia-1 (MCL-1), and a sustained resistance to a second treatment with the drug. Interestingly, the spleen tyrosine kinase (SYK) inhibitor entospletinib, and the phosphoinositide 3-kinase delta (PI3Kδ) inhibitor idelalisib, reduced T cell activation, impaired the generation of leukemic cells with this aggressive phenotype, and were able to restore CLL sensitivity to venetoclax. Our data highlight a novel combination to overcome resistance to venetoclax in CLL.
Keywords: CLL; Entospletinib-Idelalisib; Ibrutinib-Acalabrutinib; Venetoclax resistance.
© 2021. The Author(s), under exclusive licence to Springer-Verlag GmbH Germany, part of Springer Nature.
Conflict of interest statement
GC: Astrazeneca honoraria for advisory board. RFB: AbbVie and Astrazeneca honoraria for lectures and Microsules honoraria for advisory board. MRC: AbbVie honoraria for advisory board. GG: Janssen, Astrazaneca, Sanofi, Varifarma, Teva, Roche and Novartis honoraria for advisory board. MAP: Janssen, Astrazeneca, Raffo and AbbVie honoraria for lectures and Advisory boards. RG: Astrazeneca and AbbVie honoraria for lectures. The remaining authors declare no competing financial interests.
Figures



Comment in
-
"Accelerated phase" chronic lymphocytic leukemia: Still an intermediate risk disease in the era of targeted therapies.Hematol Oncol. 2022 Oct;40(4):805-808. doi: 10.1002/hon.2985. Epub 2022 Mar 8. Hematol Oncol. 2022. PMID: 35246868 No abstract available.
References
-
- Roberts AW, Davids MS, Pagel JM, Kahl BS, Puvvada SD, Gerecitano JF, Kipps TJ, Anderson MA, Brown JR, Gressick L, Wong S, Dunbar M, Zhu M, Desai MB, Cerri E, Heitner Enschede S, Humerickhouse RA, Wierda WG, Seymour JF. Targeting BCL2 with venetoclax in relapsed chronic lymphocytic Leukemia. N Engl J Med. 2016;374(4):311–322. doi: 10.1056/NEJMoa1513257. - DOI - PMC - PubMed
-
- Fischer K, Al-Sawaf O, Bahlo J, Fink AM, Tandon M, Dixon M, Robrecht S, Warburton S, Humphrey K, Samoylova O, Liberati AM, Pinilla-Ibarz J, Opat S, Sivcheva L, Le Du K, Fogliatto LM, Niemann CU, Weinkove R, Robinson S, Kipps TJ, Boettcher S, Tausch E, Humerickhouse R, Eichhorst B, Wendtner CM, Langerak AW, Kreuzer KA, Ritgen M, Goede V, Stilgenbauer S, Mobasher M, Hallek M. Venetoclax and obinutuzumab in patients with CLL and coexisting conditions. N Engl J Med. 2019;380(23):2225–2236. doi: 10.1056/NEJMoa1815281. - DOI - PubMed
-
- Mato AR, Thompson M, Allan JN, Brander DM, Pagel JM, Ujjani CS, Hill BT, Lamanna N, Lansigan F, Jacobs R, Shadman M, Skarbnik AP, Pu JJ, Barr PM, Sehgal AR, Cheson BD, Zent CS, Tuncer HH, Schuster SJ, Pickens PV, Shah NN, Goy A, Winter AM, Garcia C, Kennard K, Isaac K, Dorsey C, Gashonia LM, Singavi AK, Roeker LE, Zelenetz A, Williams A, Howlett C, Weissbrot H, Ali N, Khajavian S, Sitlinger A, Tranchito E, Rhodes J, Felsenfeld J, Bailey N, Patel B, Burns TF, Yacur M, Malhotra M, Svoboda J, Furman RR, Nabhan C. Real-world outcomes and management strategies for venetoclax-treated chronic lymphocytic leukemia patients in the United States. Haematologica. 2018;103(9):1511–1517. doi: 10.3324/haematol.2018.193615. - DOI - PMC - PubMed
-
- Elias EE, Almejun MB, Colado A, Cordini G, Vergara-Rubio M, Podaza E, Risnik D, Cabrejo M, Fernandez-Grecco H, Bezares RF, Custidiano MDR, Sanchez-Avalos JC, Vicente A, Garate GM, Borge M, Giordano M, Gamberale R. Autologous T-cell activation fosters ABT-199 resistance in chronic lymphocytic leukemia: rationale for a combined therapy with SYK inhibitors and anti-CD20 monoclonal antibodies. Haematologica. 2018;103(10):e458–e461. doi: 10.3324/haematol.2018.188680. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
