

Assessment of the Effect of Filgotinib on the Pharmacokinetics of Atorvastatin, Pravastatin, and Rosuvastatin in Healthy Adult Participants
- PMID: 34468080
- PMCID: PMC9293227
- DOI: 10.1002/cpdd.1015
Assessment of the Effect of Filgotinib on the Pharmacokinetics of Atorvastatin, Pravastatin, and Rosuvastatin in Healthy Adult Participants
Abstract
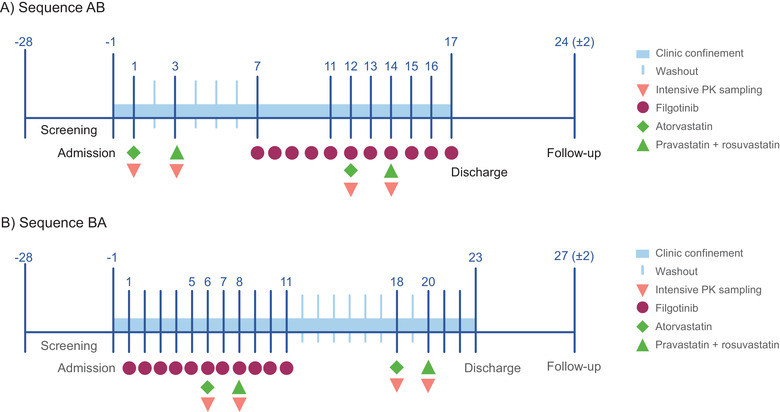
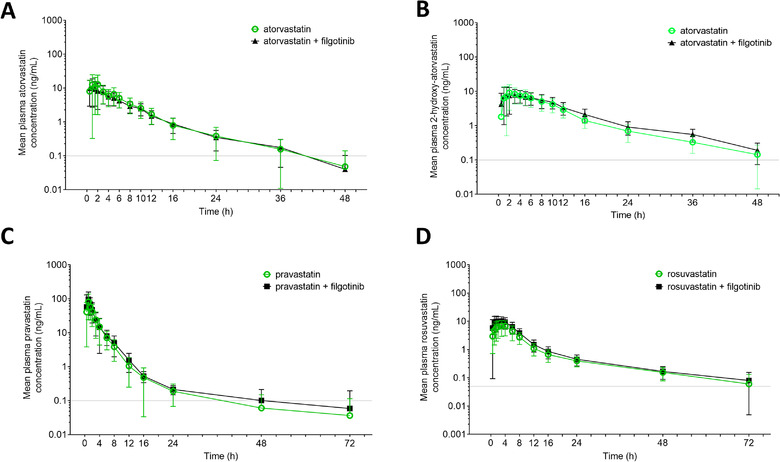
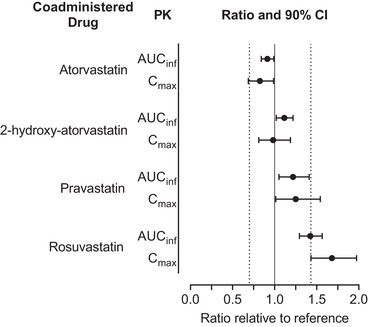
Filgotinib, an oral Janus kinase-1 preferential inhibitor, is approved in Europe and Japan for adults with rheumatoid arthritis. Patients with rheumatoid arthritis are at higher risk of cardiovascular morbidity/mortality; thus, it is important to understand potential drug-drug interactions of filgotinib with lipid-lowering agents. This open-label, randomized, 2-way crossover study evaluated the pharmacokinetics of atorvastatin, pravastatin, and rosuvastatin with and without filgotinib coadministration. Healthy participants (N = 27) received single doses of atorvastatin (40 mg) and of a pravastatin (40 mg)/rosuvastatin (10 mg) cocktail-alone or with filgotinib (200 mg once daily for 11 days)-on 2 different occasions with washout in between. Serial pharmacokinetic blood samples were collected, and safety was assessed. Pharmacokinetic parameters were evaluated using 90% confidence intervals (CI) of the geometric least-squares mean (GLSM) ratio of the test treatment (statin coadministration with filgotinib) vs statin alone, with prespecified lack-of-interaction bounds of 0.70 to 1.43. Coadministration of filgotinib did not affect atorvastatin area under the plasma concentration-time curve extrapolated to infinity (AUCinf ; [GLSM ratios (90% CI): 0.91 (0.84-0.99)]), but maximum concentration [Cmax ] was slightly lower [0.82 (0.69-0.99)]. The exposure of 2-hydroxy-atorvastatin was unaffected (GLSM ratios [90% CI], 0.98 [0.81-1.19] for Cmax ; 1.11 [1.02-1.22] for AUCinf ). Pravastatin AUCinf was also unaffected (GLSM ratios, 1.22 [1.05-1.41], but Cmax was slightly higher 1.25 [1.01-1.54]). Rosuvastatin exposure was moderately higher with filgotinib coadministration-GLSM ratios (90% CI), 1.68 (1.43-1.97) for Cmax ; 1.42 (1.30-1.57) for AUCinf -but this was not considered clinically relevant. These results indicate that filgotinib has no clinically meaningful effect on exposure of atorvastatin, pravastatin, or rosuvastatin.
Keywords: clinical pharmacology; drug-drug interactions; pharmacokinetics and drug metabolism; pharmacology; rheumatology.
© 2021 Gilead Sciences, Inc. Clinical Pharmacology in Drug Development published by Wiley Periodicals LLC on behalf of American College of Clinical Pharmacology.
Conflict of interest statement
K.A., C.N., Q.G., M.A., T.T., and A.O. are employees and shareholders of Gilead Sciences, Inc. Writing and editorial support was provided by Kathleen Pieper, PhD, and Helen Rodgers, PhD, of AlphaScientia, LLC, and was funded by Gilead Sciences, Inc. This work was supported by Gilead Sciences, Inc.
Figures
References
-
- Piepoli MF, Hoes AW, Agewall S, et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur Heart J. 2016;37:2315‐2381. - PMC - PubMed
-
- Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. Circulation. 2019;139:e1082‐e143. - PMC - PubMed
-
- Hollan I, Ronda N, Dessein P, et al. Lipid management in rheumatoid arthritis: a position paper of the Working Group on Cardiovascular Pharmacotherapy of the European Society of Cardiology. Eur Heart J Cardiovasc Pharmacother. 2020;6:104‐114. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
