

Sociodemographic, Clinical, and Treatment-Related Factors Associated With Hyperglycemic Crises Among Adults With Type 1 or Type 2 Diabetes in the US From 2014 to 2020
- PMID: 34468753
- PMCID: PMC8411297
- DOI: 10.1001/jamanetworkopen.2021.23471
Sociodemographic, Clinical, and Treatment-Related Factors Associated With Hyperglycemic Crises Among Adults With Type 1 or Type 2 Diabetes in the US From 2014 to 2020
Abstract
Importance: Hyperglycemic crises (ie, diabetic ketoacidosis [DKA] and hyperglycemic hyperosmolar state [HHS]) are life-threatening acute complications of diabetes. Efforts to prevent these events at the population level have been hindered by scarce granular data and difficulty in identifying individuals at highest risk.
Objective: To assess sociodemographic, clinical, and treatment-related factors associated with hyperglycemic crises in adults with type 1 or type 2 diabetes in the US from 2014 to 2020.
Design, setting, and participants: This retrospective cohort study analyzed administrative claims and laboratory results for adults (aged ≥18 years) with type 1 or type 2 diabetes from the OptumLabs Data Warehouse from January 1, 2014, through December 31, 2020.
Main outcomes and measures: Rates of emergency department or hospital visits with a primary diagnosis of DKA or HHS (adjusted for age, sex, race/ethnicity, and region, and for year when calculating annualized rates) were calculated separately for patients with type 1 diabetes and type 2 diabetes. The associations of sociodemographic factors (age, sex, race/ethnicity, region, and income), clinical factors (comorbidities), and treatment factors (glucose-lowering medications, hemoglobin A1c) with DKA or HHS in patients with type 1 or type 2 diabetes were assessed using negative binomial regression.
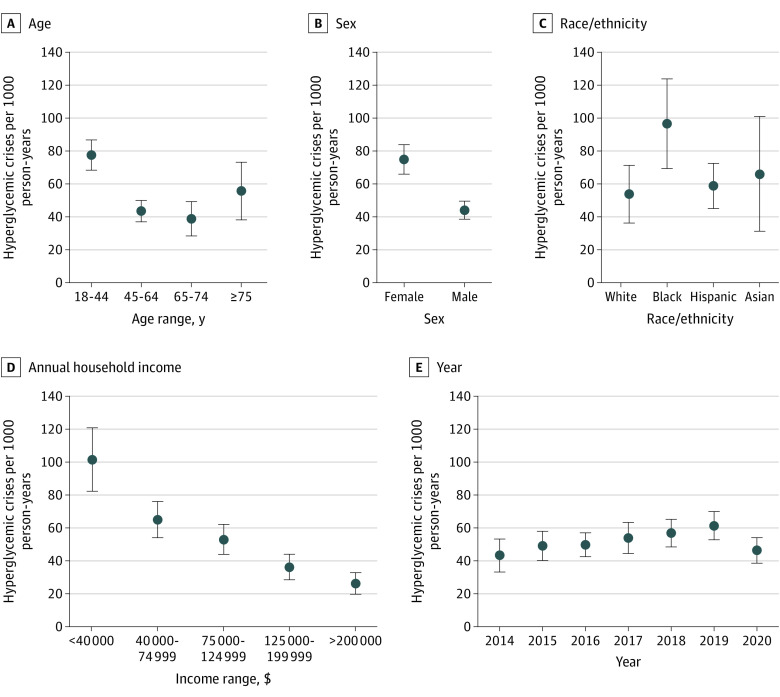
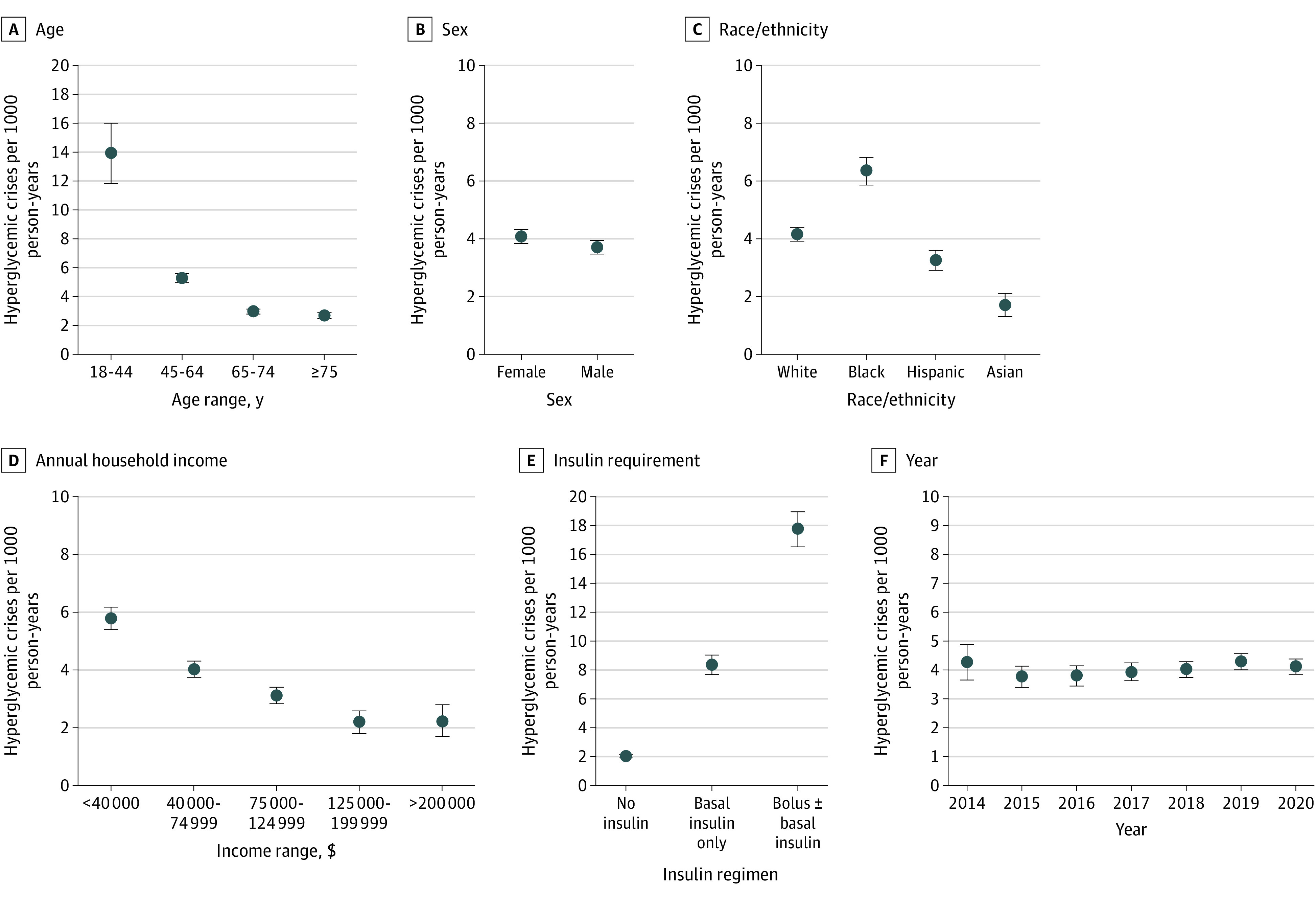
Results: Among 20 156 adults with type 1 diabetes (mean [SD] age, 46.6 [16.5] years; 51.2% male; 72.6% White race/ethnicity) and 796 382 with type 2 diabetes (mean [SD] age, 65.6 [11.8] years; 50.3% female; 54.4% White race/ethnicity), adjusted rates of hyperglycemic crises were 52.69 per 1000 person-years (95% CI, 48.26-57.12 per 1000 person-years) for type 1 diabetes and 4.04 per 1000 person-years (95% CI, 3.88-4.21 per 1000 person-years) for type 2 diabetes. In both groups, factors associated with the greatest hyperglycemic crisis risk were low income (≥$200 000 vs <$40 000: type 1 diabetes incidence risk ratio [IRR], 0.61 [95% CI, 0.46-0.81]; type 2 diabetes IRR, 0.69 [95% CI, 0.56-0.86]), Black race/ethnicity (vs White race/ethnicity: type 1 diabetes IRR, 1.33 [95% CI, 1.01-1.74]; type 2 diabetes IRR, 1.18 [95% CI, 1.09-1.27]), high hemoglobin A1c level (≥10% vs 6.5%-6.9%: type 1 diabetes IRR, 7.81 [95% CI, 5.78-10.54]; type 2 diabetes IRR, 7.06 [95% CI, 6.26-7.96]), history of hyperglycemic crises (type 1 diabetes IRR, 7.88 [95% CI, 6.06-9.99]; type 2 diabetes IRR, 17.51 [95% CI, 15.07-20.34]), severe hypoglycemia (type 1 diabetes IRR, 2.77 [95% CI, 2.15-3.56]; type 2 diabetes IRR, 4.18 [95% CI, 3.58-4.87]), depression (type 1 diabetes IRR, 1.62 [95% CI, 1.37-1.92]; type 2 diabetes IRR, 1.46 [95% CI, 1.34-1.59]), neuropathy (type 1 diabetes IRR, 1.64 [95% CI, 1.39-1.93]; type 2 diabetes IRR, 1.25 [95% CI, 1.17-1.34]), and nephropathy (type 1 diabetes IRR, 1.22 [95% CI, 1.01-1.48]; type 2 diabetes IRR, 1.23 [95% CI, 1.14-1.33]). Age had a U-shaped association with hyperglycemic crisis risk in patients with type 1 diabetes (compared with patients aged 18-44 years: 45-64 years IRR, 0.72 [95% CI, 0.59-0.87]; 65-74 years IRR, 0.62 [95% CI, 0.47-0.80]; ≥75 years IRR, 0.96 [95% CI, 0.66-1.38]). In type 2 diabetes, risk of hyperglycemic crises decreased progressively with age (45-64 years IRR, 0.57 [95% CI, 0.51-0.63]; 65-74 years IRR, 0.44 [95% CI, .39-0.49]; ≥75 years IRR, 0.41 [95% CI, 0.36-0.47]). In patients with type 2 diabetes, higher risk was associated with sodium-glucose cotransporter 2 inhibitor therapy (IRR, 1.30; 95% CI, 1.14-1.49) and insulin dependency (compared with regimens with bolus insulin: regimens with basal insulin only, IRR, 0.69 [95% CI, 0.63-0.75]; and without any insulin, IRR, 0.36 [95% CI, 0.33-0.40]).
Conclusions and relevance: In this cohort study, younger age, Black race/ethnicity, low income, and poor glycemic control were associated with an increased risk of hyperglycemic crises. The findings suggest that multidisciplinary interventions focusing on groups at high risk for hyperglycemic crises are needed to prevent these dangerous events.
Conflict of interest statement
Figures
References
-
- Centers for Disease Control and Prevention . National Diabetes Statistics Report, 2020. US Department of Health and Human Services, Centers for Disease Control and Prevention; 2020.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
