

Association between Preferred Language and Risk of Severe Acute Respiratory Syndrome Coronavirus 2 Infection in Children in the United States
- PMID: 34469330
- PMCID: PMC8592181
- DOI: 10.4269/ajtmh.21-0779
Association between Preferred Language and Risk of Severe Acute Respiratory Syndrome Coronavirus 2 Infection in Children in the United States
Abstract
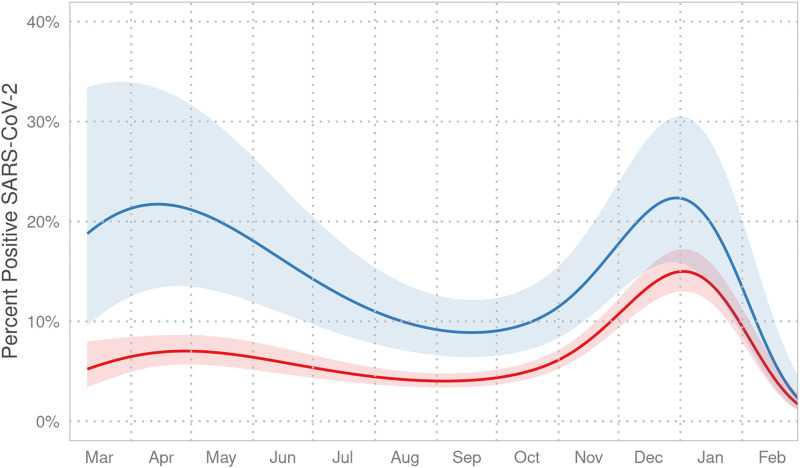
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic has had a disproportionate impact on Black, Hispanic, and other individuals of color, although data on the effect of a person's language on SARS-CoV-2 infection are limited. Considering the barriers suffered by immigrants and non-English-speaking families, we tested whether children with a preferred language other than English was associated with SARS-CoV-2 infection. Children from families with a preferred language other than English had a higher predicted probability of SARS-CoV-2 test positivity (adjusted odds ratio, 3.76; 95% CI, 2.07-6.67) during the first wave of the pandemic. This discrepancy continued into the second wave (adjusted odds ratio, 1.64; 95% CI, 1.10-2.41), although the difference compared with families who prefer to speak English decreased over time. These findings suggest that children from non-English-speaking families are at increased risk of SARS-CoV-2 infection, and efforts to reverse systemic inequities causing this increased risk are needed.
Figures
References
-
- Azar KMJ, Shen Z, Romanelli RJ, Locjhart SH, Smits K, Robinson S, Brown S, Pressman AR, 2020. Disparities in outcomes among COVID-19 patients in a large health care system in California. Health Aff 39: 1253–1262. - PubMed
-
- Goyal MK, Simpson JN, Boyle MD, Badolato GM, Delaney M, McCarter R, Cora-Bramble D, 2020. Racial and/or ethnic and socioeconomic disparities of SARS-CoV-2 infection among children. Pediatrics 146: e2020009951. - PubMed
-
- Bixler D, Miller A, Mattison C, Taylor B, Komatsu K, Peterson Pompa X, Moon S, Karmarkar E, Liu C, Openshaw J, 2020. SARS-CoV-2–associated deaths among persons aged < 21 years—United States, February 12–July 31, 2020. MMWR Morbidity Mortality Weekly Rep. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
