

Diseases of the Aorta and Kidney Disease: conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference
- PMID: 34469520
- PMCID: PMC9491875
- DOI: 10.1093/cvr/cvab287
Diseases of the Aorta and Kidney Disease: conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference
Abstract
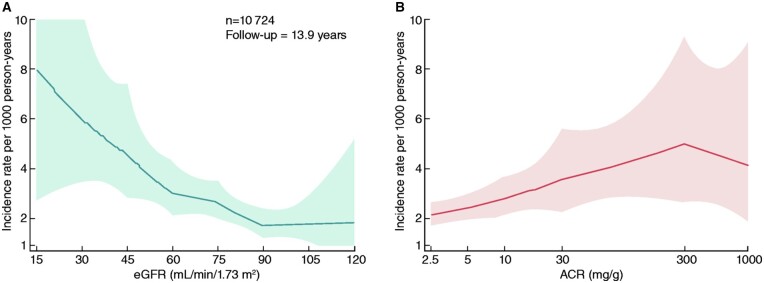
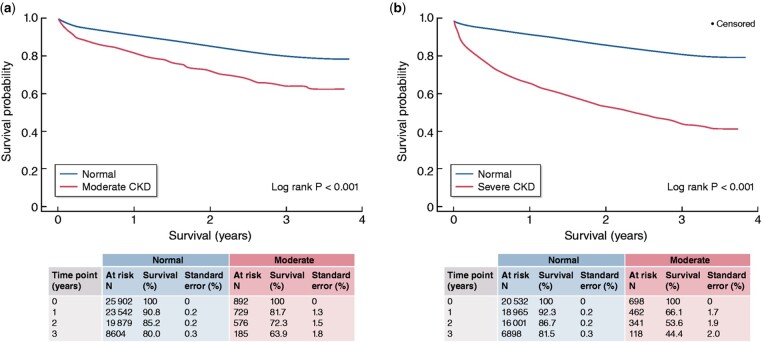
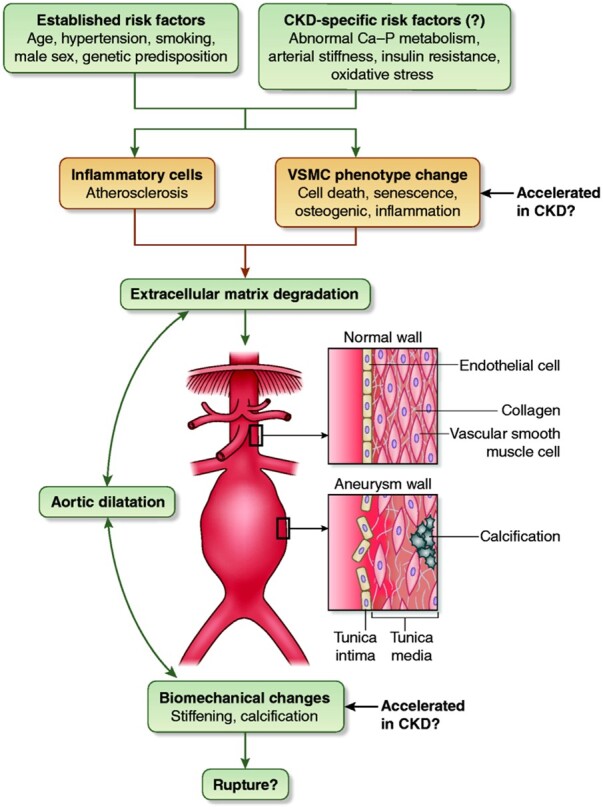
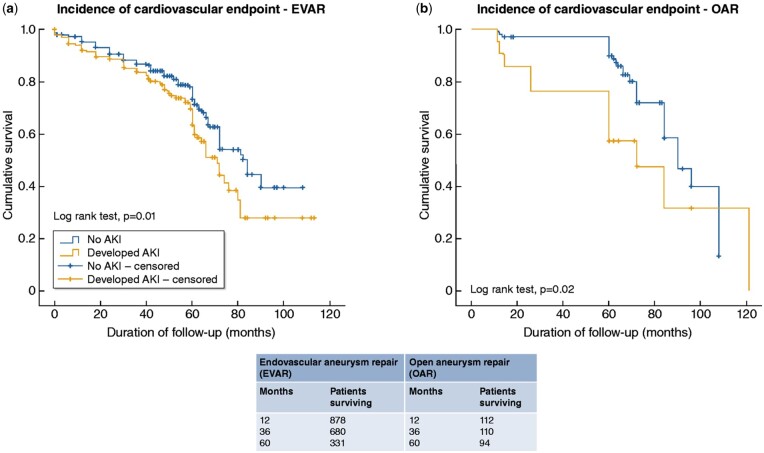
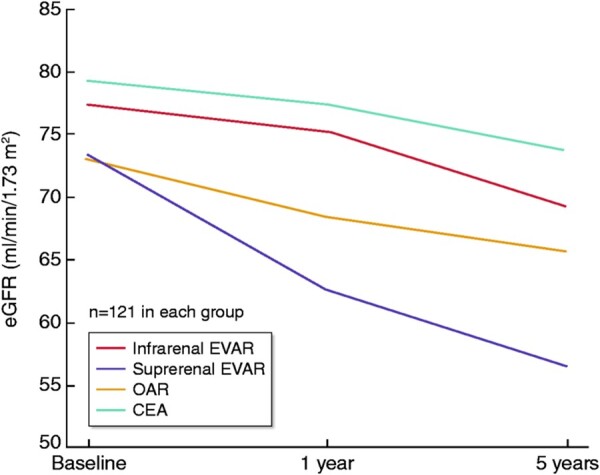
Chronic kidney disease (CKD) is an independent risk factor for the development of abdominal aortic aneurysm (AAA), as well as for cardiovascular and renal events and all-cause mortality following surgery for AAA or thoracic aortic dissection. In addition, the incidence of acute kidney injury (AKI) after any aortic surgery is particularly high, and this AKI per se is independently associated with future cardiovascular events and mortality. On the other hand, both development of AKI after surgery and the long-term evolution of kidney function differ significantly depending on the type of AAA intervention (open surgery vs. the various subtypes of endovascular repair). Current knowledge regarding AAA in the general population may not be always applicable to CKD patients, as they have a high prevalence of co-morbid conditions and an elevated risk for periprocedural complications. This summary of a Kidney Disease: Improving Global Outcomes Controversies Conference group discussion reviews the epidemiology, pathophysiology, diagnosis, and treatment of Diseases of the Aorta in CKD and identifies knowledge gaps, areas of controversy, and priorities for future research.
Keywords: Abdominal aortic aneurysm; Acute kidney injury; Aortic diseases; Aortic dissection; Chronic kidney disease.
© The Author(s) 2021. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: All authors report travel support from Kidney Disease: Improving Global Outcomes (KDIGO) for the KDIGO Controversies Conference February 2021 in Dublin, Ireland. CH declares receiving consultant fees from Abbvie, Amgen, AstraZeneca, Bayer, Corvidia, Diamedica, FibroGen, Janssen, National Heart Lung and Blood Institute (NHLBI/NIH), NxStage, Pfizer, Relypsa, Sanifit, and University of Oxford; stock equity from Boston Scientific, Bristol-Myers Squibb, General Electric, Johnson & Johnson, and Merck; research support from Amgen, AstraZeneca, Bristol-Myers Squibb, NHLBI/NIH, NIDDK/NIH, Relypsa, University of British Columbia; and author royalties from UpToDate M.J. reports educational grant from Astra-Zeneca paid to his institution. W.W. reports research grants from the U.S. National Institutes of Health paid to his institution, participation on Data Safety Monitoring Boards for studies sponsored by Akebia, Bayer, and Merck and participation in advisory boards from Akebia/Otsuka, AstraZeneca, Bayer, Eli Lilly/Boehringer Ingelsheim, Merck, Janssen, Reata, Relypsa, and Vifor Fresenius Medical Care Renal Pharma. H.R. reports research grants from Bard, Pfizer & BMS, Pluristem, Biotronic paid to his institution, consulting fees from Pluristem and Neovasc, and speaker fees from Daichi Sankyo, Diaplan, Medupdate, Stremedup, and Corvia. K.J. reports grants from National Institute for Diabetes and Digestive and Kidney Disease, consulting fees from GSK and Participation on Data Safety Monitoring Board for NIDKK. The rest of the authors report no other conflict of interest relevant to this work.
Figures
References
-
- Johansen K, Garimella P, Hicks C, Kalra PA, Kelly D, Martens S, Matsushita K, Sarafidis P, Sood M, Herzog CA, Cheung M, Jadoul M, Winkelmayer WC, Reinecke H, Conference Participants . Central and peripheral arterial diseases in chronic kidney disease: conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int 2021;100:35–48. - PMC - PubMed
-
- Cosford PA, Leng GC.. Screening for abdominal aortic aneurysm. Cochrane Database Syst Rev 2007;2:CD002945. - PubMed
-
- Svensjo S, Bjorck M, Gurtelschmid M, Djavani Gidlund K, Hellberg A, Wanhainen A.. Low prevalence of abdominal aortic aneurysm among 65-year-old Swedish men indicates a change in the epidemiology of the disease. Circulation 2011;124:1118–1123. - PubMed
-
- Barba Á, Vega de Céniga M, Estallo L, de la Fuente N, Viviens B, Izagirre M.. Prevalence of abdominal aortic aneurysm is still high in certain areas of southern Europe. Ann Vasc Surg 2013;27:1068–1073. - PubMed
-
- Svensjö S, Björck M, Wanhainen A.. Current prevalence of abdominal aortic aneurysm in 70-year-old women. Br J Surg 2013;100:367–372. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
