

Treatment of Relapsing HPV Diseases by Restored Function of Natural Killer Cells
- PMID: 34469647
- PMCID: PMC8590529
- DOI: 10.1056/NEJMoa2102715
Treatment of Relapsing HPV Diseases by Restored Function of Natural Killer Cells
Abstract
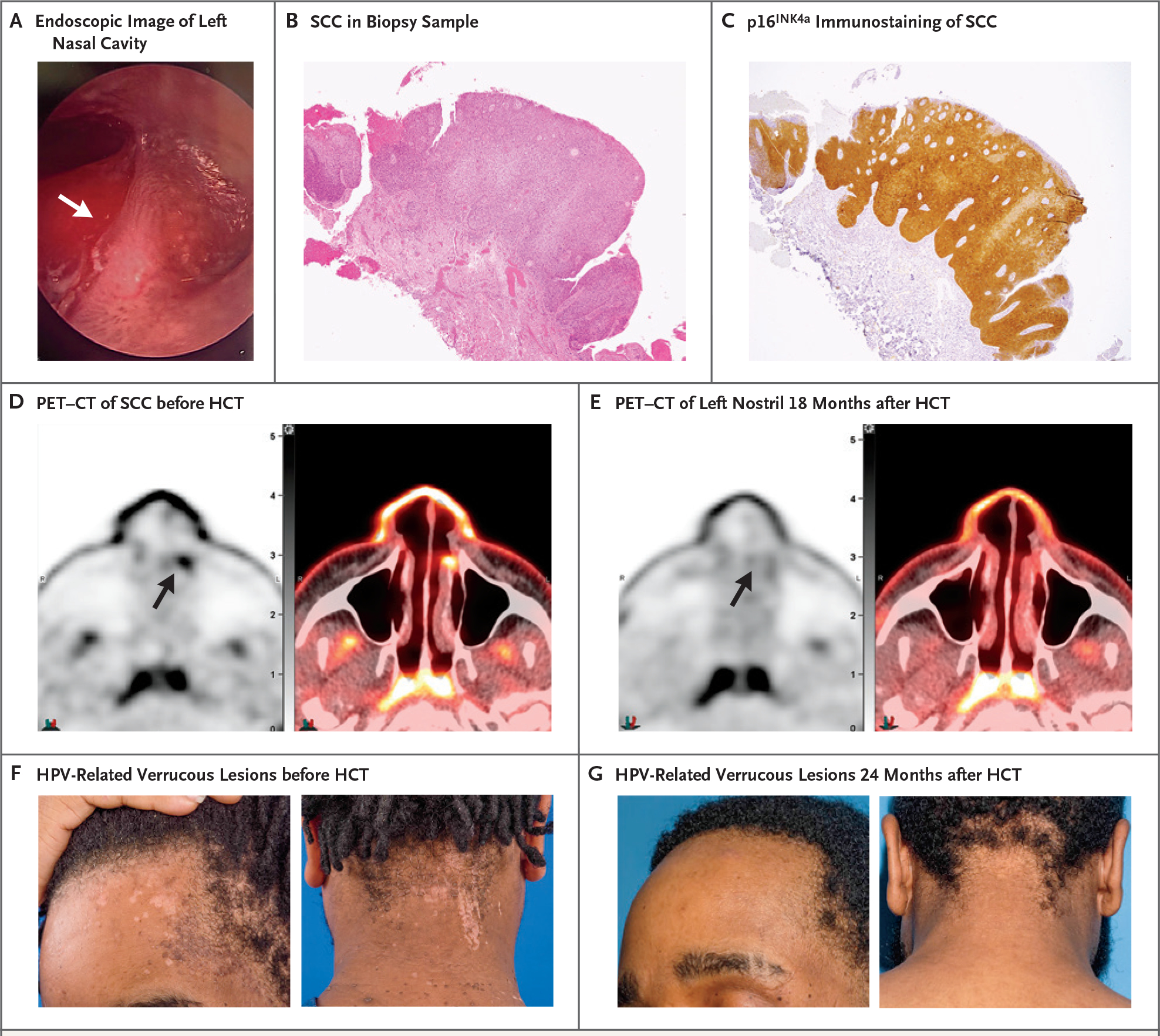
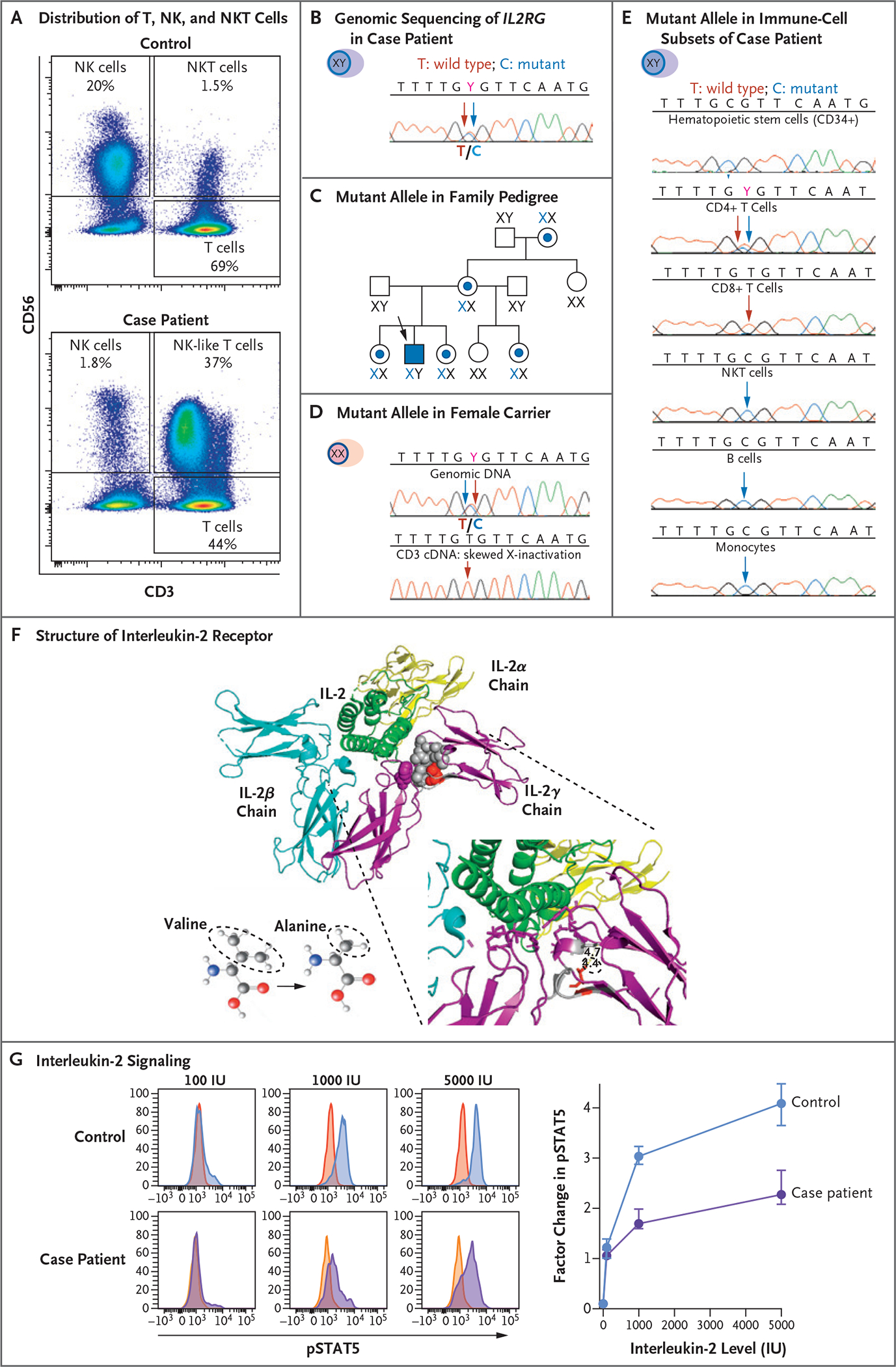
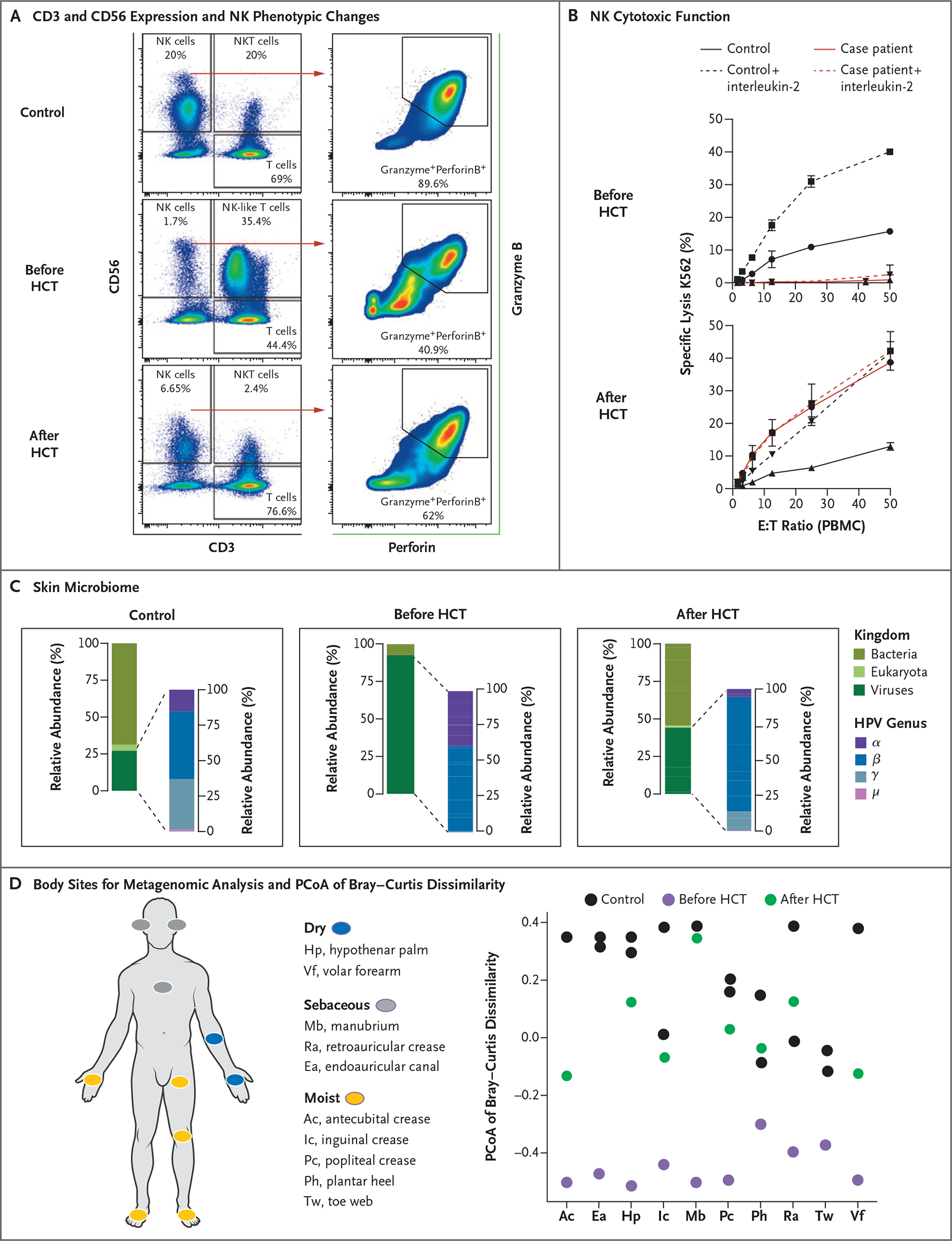
Human papillomavirus (HPV) infections underlie a wide spectrum of both benign and malignant epithelial diseases. In this report, we describe the case of a young man who had encephalitis caused by herpes simplex virus during adolescence and currently presented with multiple recurrent skin and mucosal lesions caused by HPV. The patient was found to have a pathogenic germline mutation in the X-linked interleukin-2 receptor subunit gamma gene (IL2RG), which was somatically reverted in T cells but not in natural killer (NK) cells. Allogeneic hematopoietic-cell transplantation led to restoration of NK cytotoxicity, with normalization of the skin microbiome and persistent remission of all HPV-related diseases. NK cytotoxicity appears to play a role in containing HPV colonization and the ensuing HPV-related hyperplastic or dysplastic lesions. (Funded by the National Institutes of Health and the Herbert Irving Comprehensive Cancer Center Flow Cytometry Shared Resources.).
Copyright © 2021 Massachusetts Medical Society.
Figures
References
-
- Lei J, Ploner A, Elfström KM, et al. HPV vaccination and the risk of invasive cervical cancer. N Engl J Med 2020;383: 1340–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources