

Second asymptomatic carotid surgery trial (ACST-2): a randomised comparison of carotid artery stenting versus carotid endarterectomy
- PMID: 34469763
- PMCID: PMC8473558
- DOI: 10.1016/S0140-6736(21)01910-3
Second asymptomatic carotid surgery trial (ACST-2): a randomised comparison of carotid artery stenting versus carotid endarterectomy
Abstract
Background: Among asymptomatic patients with severe carotid artery stenosis but no recent stroke or transient cerebral ischaemia, either carotid artery stenting (CAS) or carotid endarterectomy (CEA) can restore patency and reduce long-term stroke risks. However, from recent national registry data, each option causes about 1% procedural risk of disabling stroke or death. Comparison of their long-term protective effects requires large-scale randomised evidence.
Methods: ACST-2 is an international multicentre randomised trial of CAS versus CEA among asymptomatic patients with severe stenosis thought to require intervention, interpreted with all other relevant trials. Patients were eligible if they had severe unilateral or bilateral carotid artery stenosis and both doctor and patient agreed that a carotid procedure should be undertaken, but they were substantially uncertain which one to choose. Patients were randomly allocated to CAS or CEA and followed up at 1 month and then annually, for a mean 5 years. Procedural events were those within 30 days of the intervention. Intention-to-treat analyses are provided. Analyses including procedural hazards use tabular methods. Analyses and meta-analyses of non-procedural strokes use Kaplan-Meier and log-rank methods. The trial is registered with the ISRCTN registry, ISRCTN21144362.
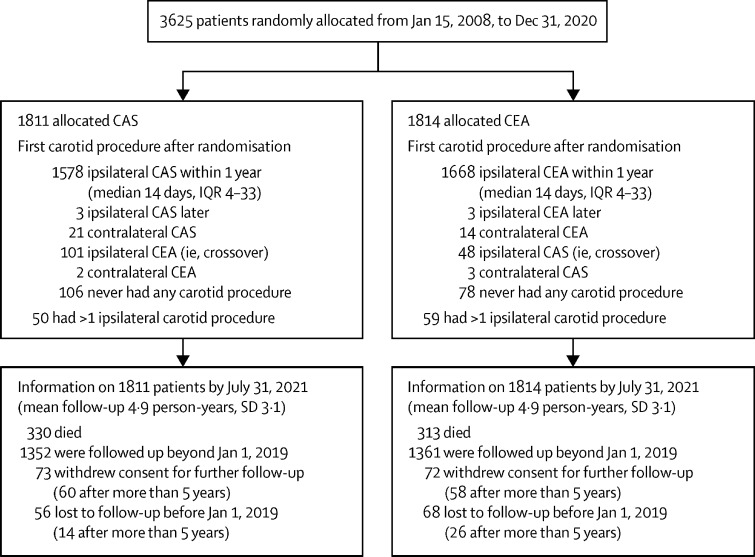
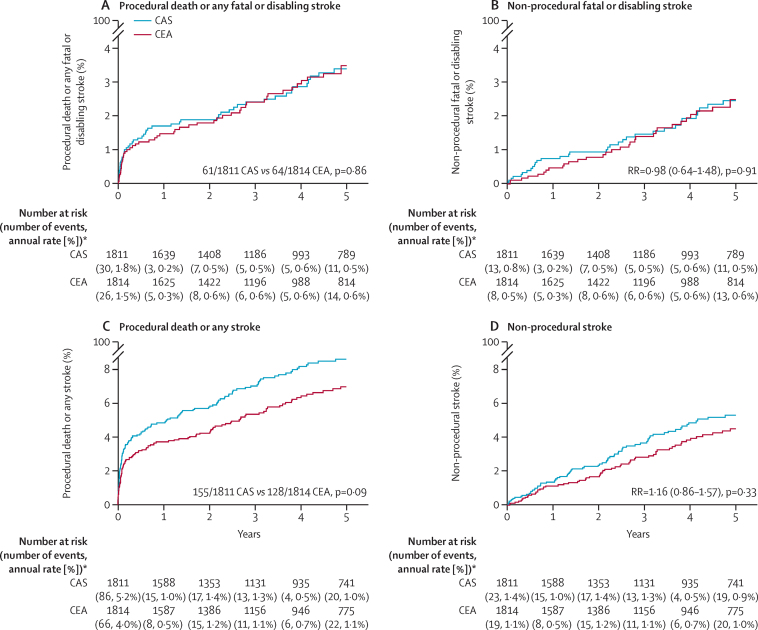
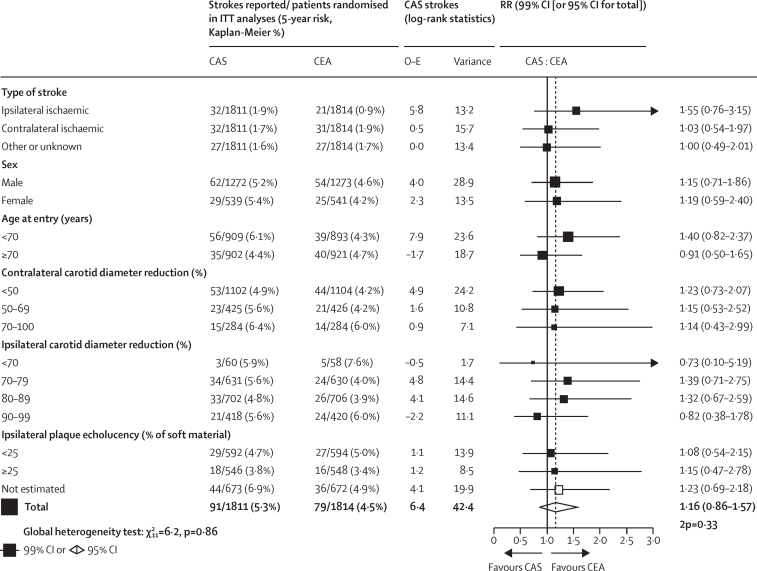
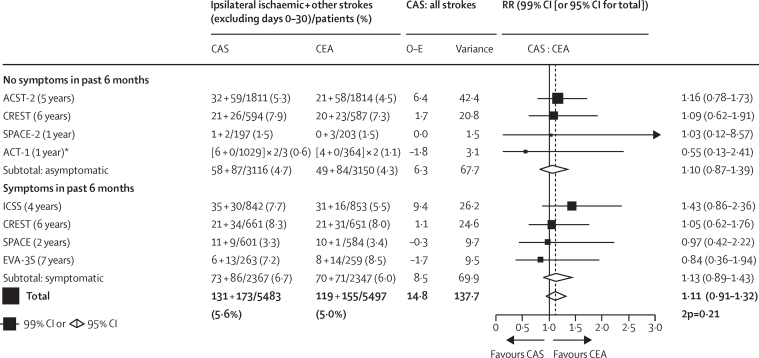
Findings: Between Jan 15, 2008, and Dec 31, 2020, 3625 patients in 130 centres were randomly allocated, 1811 to CAS and 1814 to CEA, with good compliance, good medical therapy and a mean 5 years of follow-up. Overall, 1% had disabling stroke or death procedurally (15 allocated to CAS and 18 to CEA) and 2% had non-disabling procedural stroke (48 allocated to CAS and 29 to CEA). Kaplan-Meier estimates of 5-year non-procedural stroke were 2·5% in each group for fatal or disabling stroke, and 5·3% with CAS versus 4·5% with CEA for any stroke (rate ratio [RR] 1·16, 95% CI 0·86-1·57; p=0·33). Combining RRs for any non-procedural stroke in all CAS versus CEA trials, the RR was similar in symptomatic and asymptomatic patients (overall RR 1·11, 95% CI 0·91-1·32; p=0·21).
Interpretation: Serious complications are similarly uncommon after competent CAS and CEA, and the long-term effects of these two carotid artery procedures on fatal or disabling stroke are comparable.
Funding: UK Medical Research Council and Health Technology Assessment Programme.
Copyright © 2021 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests We declare no competing interests.
Figures
Comment in
-
Intervention for asymptomatic carotid artery stenosis.Lancet. 2021 Sep 18;398(10305):1025-1027. doi: 10.1016/S0140-6736(21)01965-6. Epub 2021 Aug 29. Lancet. 2021. PMID: 34469761 No abstract available.
-
CAS and CEA have similar risks and benefits.Nat Rev Cardiol. 2021 Nov;18(11):738. doi: 10.1038/s41569-021-00622-4. Nat Rev Cardiol. 2021. PMID: 34508231 No abstract available.
-
Is stenting equivalent to endarterectomy for asymptomatic carotid stenosis?Lancet. 2022 Mar 19;399(10330):1114-1115. doi: 10.1016/S0140-6736(21)02498-3. Lancet. 2022. PMID: 35305736 No abstract available.
-
Is stenting equivalent to endarterectomy for asymptomatic carotid stenosis?Lancet. 2022 Mar 19;399(10330):1115-1116. doi: 10.1016/S0140-6736(21)02497-1. Lancet. 2022. PMID: 35305737 No abstract available.
References
-
- Cole TS, Mezher AW, Catapano JS. Nationwide trends in carotid endarterectomy and carotid artery stenting in the post-CREST era. Stroke. 2020;51:579–587. - PubMed
-
- Venermo M, Wang G, Sedrakyan A. Editor's choice—carotid stenosis treatment: variation in international practice patterns. Eur J Vasc Endovasc Surg. 2017;53:511–519. - PubMed
-
- Institut für Qualitätssicherung und Transparenz im Gesundheitswesen (IQTiG) Karotis-Revaskularisation. https://iqtig.org/qs-verfahren/qs-karotis/
-
- Halliday A, Peto R, Bulbulia R. Carotid artery surgery to reduce long-term stroke rates: individual patient data meta-analysis of the randomised trials in asymptomatic patients. SSRN. 2021 https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3909921 published online Aug 23. (preprint).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
