

Traumatic Brachial Plexus Injury in Indonesia: An Experience from a Developing Country
- PMID: 34470060
- PMCID: PMC9470278
- DOI: 10.1055/s-0041-1735507
Traumatic Brachial Plexus Injury in Indonesia: An Experience from a Developing Country
Abstract
Background: Brachial plexus injuries (BPI) cause severe physical disability and major psycho-socioeconomic burden. Although various countries have reported BPI incidence, the data from Indonesia as the fourth most populated country in the world remains unknown. We aim to assess the distribution of traumatic BPI, patients' characteristics, and treatment modalities in Indonesia.
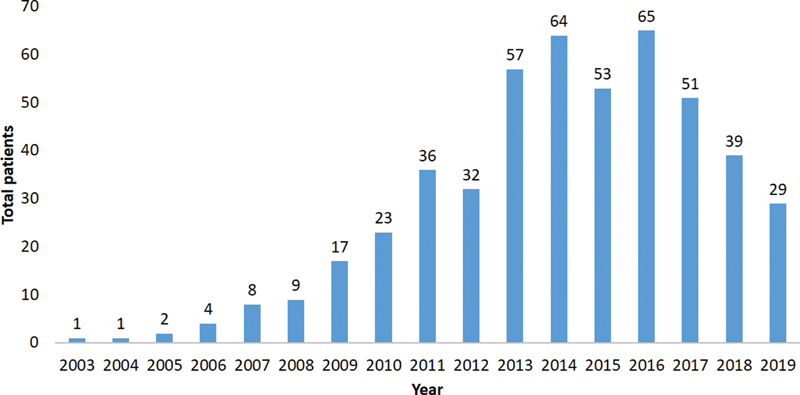
Methods: A retrospective investigation was performed comprising 491 BPI patients at a tertiary referral hospital in Indonesia from January 2003 to October 2019. Demographic and outcomes data were retrieved from medical records.
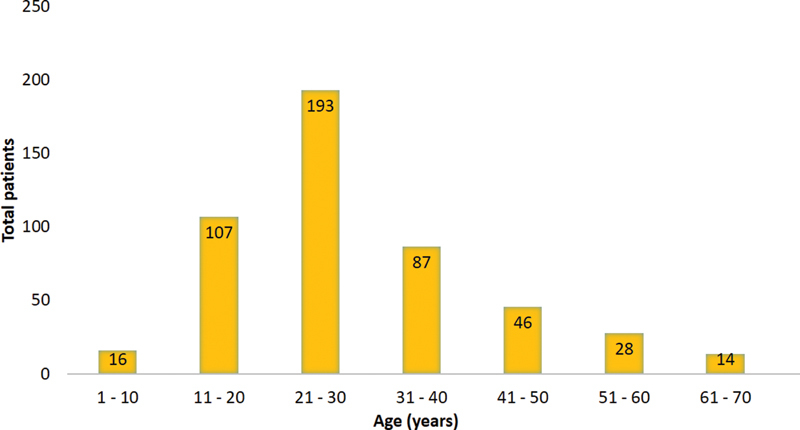
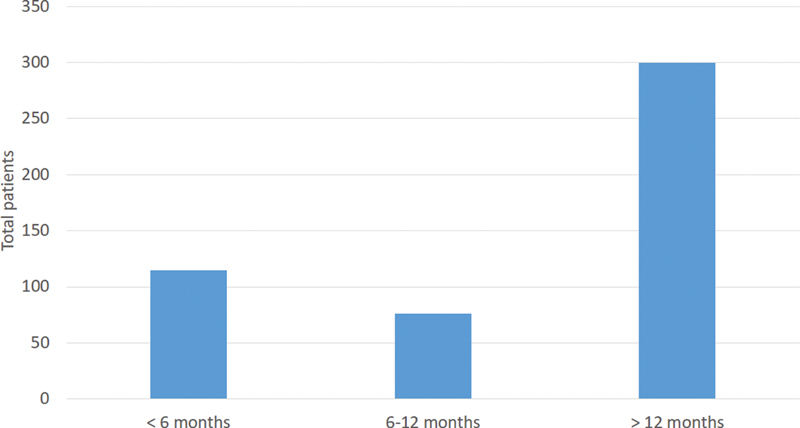
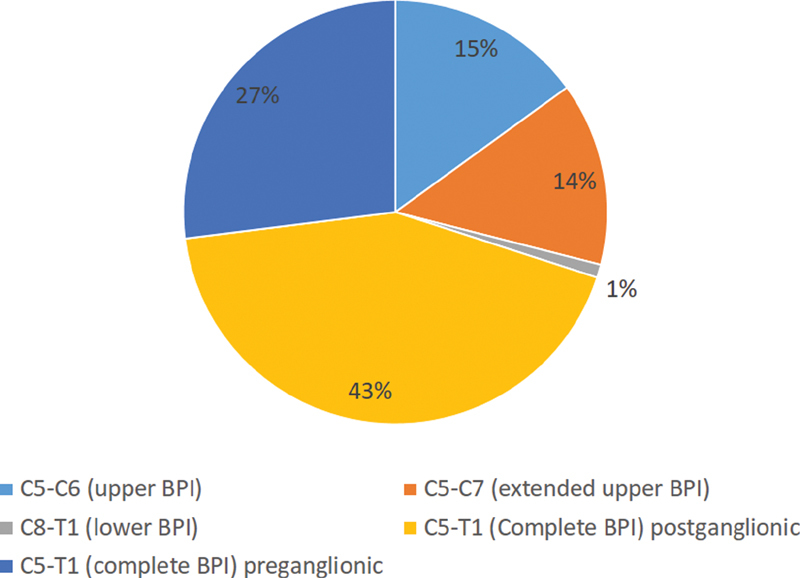
Results: The average BPI patients' age was 27.3 ± 11.6 years old, with a male/female ratio of 4.6:1. Motorcycle accidents caused the majority (76.1%) of all BPI cases. Concomitant injuries were present in 62.3% of patients, dominated by fractures (57.1%) and brain injuries (25.4%). BPI lesion type was classified into complete (C5-T1, observed in 70% patients), upper (C5-C6, in 15% patients), extended upper (C5-C7, in 14% patients), and lower type (C8-T1, in 1% patients). The average time to surgery was 16.8 months (range 1-120 months), with the majority (76.6%) of the patients was operated on six months after the trauma. Free functional muscle transfer (FFMT) was the most common procedure performed (37%). We also analyzed the functional outcomes (active range of motion (AROM) and muscle power), DASH (Disabilities of the Arm, Shoulder, and Hand) score, and VAS (Visual Analogue Scale) across four most frequent procedures involving nerve reconstruction (FFMT, nerve transfer, external neurolysis, and nerve grafting). We found that FFMT was significantly better than nerve transfer in terms of DASH score and VAS (p = 0.000 and p = 0.016, respectively) in complete BPI (C5-T1). Moreover, we also found that nerve grafting resulted in a significantly better shoulder abduction AROM than nerve transfer and external neurolysis in extended upper BPI (C5-C7) (p = 0.033 and p = 0.033, respectively). Interestingly, no significant differences were observed in other measurements.
Conclusion: This study provides an overview of traumatic BPI patients in a single tertiary trauma center in Indonesia, expressing the profile of their characteristics and functional outcomes after surgical procedures.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Conflict of interest statement
The authors declare that they have no conflict of interest.Each author certifies that he or she has no commercial associations (e.g., consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article
Figures

Similar articles
-
What is the Elbow Flexion Strength After Free Functional Gracilis Muscle Transfer for Adult Traumatic Complete Brachial Plexus Injuries?Clin Orthop Relat Res. 2022 Dec 1;480(12):2392-2405. doi: 10.1097/CORR.0000000000002311. Epub 2022 Aug 24. Clin Orthop Relat Res. 2022. PMID: 36001032 Free PMC article.
-
Management of Adult Traumatic Brachial Plexus Injury.Mymensingh Med J. 2023 Apr;32(2):437-447. Mymensingh Med J. 2023. PMID: 37002755
-
Results of grafting the anterior and posterior divisions of the upper trunk in complete palsies of the brachial plexus.J Hand Surg Am. 2008 Nov;33(9):1529-40. doi: 10.1016/j.jhsa.2008.06.007. J Hand Surg Am. 2008. PMID: 18984335
-
Gracilis free muscle transfer for restoration of function after complete brachial plexus avulsion.Neurosurg Focus. 2004 May 15;16(5):E8. doi: 10.3171/foc.2004.16.5.9. Neurosurg Focus. 2004. PMID: 15174828 Review.
-
Surgical reconstructions for adult brachial plexus injuries. Part I: Treatments for combined C5 and C6 injuries, with or without C7 injuries.Injury. 2020 Apr;51(4):787-803. doi: 10.1016/j.injury.2020.02.076. Epub 2020 Feb 17. Injury. 2020. PMID: 32156416 Review.
Cited by
-
Clinical and functional outcome after different surgical approaches for brachial plexus injuries: Cohort study.Ann Med Surg (Lond). 2022 May 10;78:103714. doi: 10.1016/j.amsu.2022.103714. eCollection 2022 Jun. Ann Med Surg (Lond). 2022. PMID: 35620046 Free PMC article.
-
The Relationship Between Patient Factors and Clinical Outcomes of Free Functional Muscle Transfer in Patients with Complete Traumatic Brachial Plexus Injury.Orthop Res Rev. 2022 Jul 5;14:225-233. doi: 10.2147/ORR.S367499. eCollection 2022. Orthop Res Rev. 2022. PMID: 35818627 Free PMC article.
-
Validity and Reliability of Prognosis Brachial Plexus Injury Score for Traumatic Brachial Plexus Injury.Clin Orthop Surg. 2023 Feb;15(1):153-158. doi: 10.4055/cios22168. Epub 2022 Oct 7. Clin Orthop Surg. 2023. PMID: 36778991 Free PMC article.
-
The Epidemiology of Traumatic Brachial Plexus Injuries in England and Wales-A 32-Year Review.JB JS Open Access. 2025 Mar 18;10(1):e24.00105. doi: 10.2106/JBJS.OA.24.00105. eCollection 2025 Jan-Mar. JB JS Open Access. 2025. PMID: 40104246 Free PMC article.
-
What is the Elbow Flexion Strength After Free Functional Gracilis Muscle Transfer for Adult Traumatic Complete Brachial Plexus Injuries?Clin Orthop Relat Res. 2022 Dec 1;480(12):2392-2405. doi: 10.1097/CORR.0000000000002311. Epub 2022 Aug 24. Clin Orthop Relat Res. 2022. PMID: 36001032 Free PMC article.
References
-
- Bonham C, Greaves I.Brachial plexus injuries Trauma 20111304353–363.Available at:https://journals.sagepub.com/doi/10.1177/1460408611405298
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
