

Needs-led human resource planning for Sierra Leone in support of oral health
- PMID: 34470631
- PMCID: PMC8411531
- DOI: 10.1186/s12960-021-00623-x
Needs-led human resource planning for Sierra Leone in support of oral health
Abstract
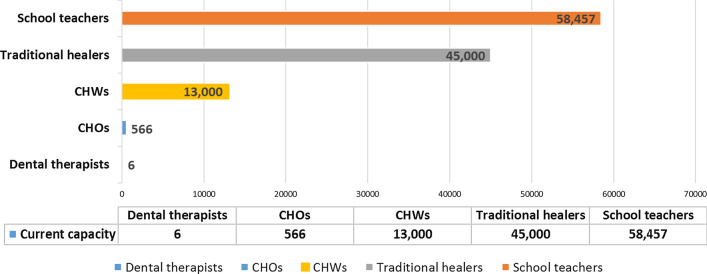
Background: In Sierra Leone (SL), a low-income country in West Africa, dental care is very limited, largely private, and with services focused in the capital Freetown. There is no formal dental education. Ten dentists supported by a similar number of dental care professionals (DCPs) serve a population of over 7.5 million people. The objective of this research was to estimate needs-led requirements for dental care and human resources for oral health to inform capacity building, based on a national survey of oral health in SL.
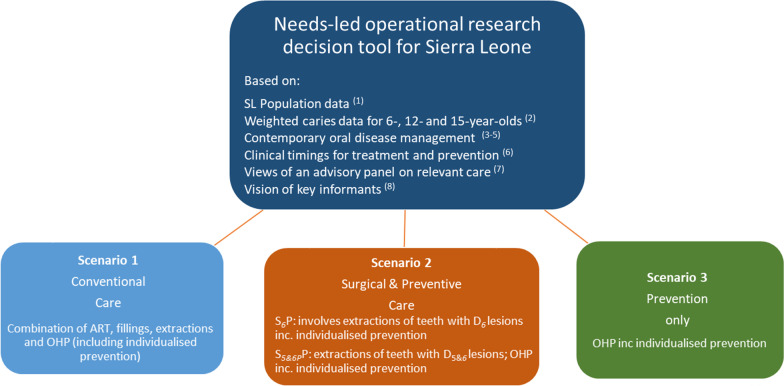
Methods: A dedicated operational research (OR) decision tool was constructed in Microsoft Excel to support this project. First, total treatment needs were estimated from our national epidemiological survey data for three key ages (6, 12 and 15 years), collected using the 'International Caries Classification and Management System (ICCMS)' tool. Second, oral health needs were extrapolated to whole population levels for each year-group, based on census demographic data. Third, full time equivalent (FTE) workforce capacity needs were estimated for mid-level providers in the form of Dental Therapists (DTs) and non-dental personnel based on current oral disease management approaches and clinical timings for treatment procedures. Fourth, informed by an expert panel, three oral disease management scenarios were explored for the national population: (1) Conventional care (CC): comprising oral health promotion (including prevention), restorations and tooth extraction; (2) Surgical and Preventive care (S5&6P and S6P): comprising oral health promotion (inc. prevention) and tooth extraction (D5 and D6 together, & at D6 level only); and (3) Prevention only (P): consisting of oral health promotion (inc. prevention). Fifth, the findings were extrapolated to the whole population based on demography, assuming similar levels of treatment need.
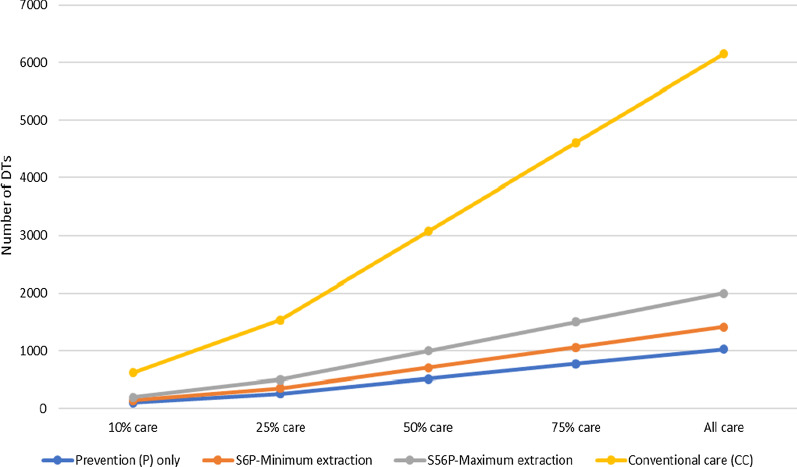
Results: To meet the needs of a single year-group of childrens' needs, an average of 163 DTs (range: 133-188) would be required to deliver Conventional care (CC); 39 DTs (range: 30-45) to deliver basic Surgical and Preventive care (S6P); 54 DTs for more extended Surgical and Preventive care (S5&6P) (range 38-68); and 27 DTs (range: 25-32) to deliver Prevention only (P). When scaled up to the total population, an estimated 6,147 DTs (range: 5,565-6,870) would be required to deliver Conventional care (CC); 1,413 DTs (range: 1255-1438 DTs) to deliver basic Surgical and Preventive care (S6P); 2,000 DTs (range 1590-2236) for more extended Surgical and Preventive care (S5&6P) (range 1590-2236); and 1,028 DTs to deliver Prevention only (P) (range: 1016-1046). Furthermore, if oral health promotion activities, including individualised prevention, could be delivered by non-dental personnel, then the remaining surgical care could be delivered by 385 DTs (range: 251-488) for the S6P scenario which was deemed as the minimum basic baseline service involving extracting all teeth with extensive caries into dentine. More realistically, 972 DTs (range: 586-1179) would be needed for the S5&6P scenario in which all teeth with distinctive and extensive caries into dentine are extracted.
Conclusion: The study demonstrates the huge dental workforce needs required to deliver even minimal oral health care to the Sierra Leone population. The gap between the current workforce and the oral health needs of the population is stark and requires urgent action. The study also demonstrates the potential for contemporary epidemiological tools to predict dental treatment needs and inform workforce capacity building in a low-income country, exploring a range of solutions involving mid-level providers and non-dental personnel.
Keywords: Atraumatic restorative treatment; Dental therapists; Dental workforce; ICCMS; ICDAS; Low-income countries; Operational research; Oral health; Oral health needs; Oral health workforce; Tooth extraction; Treatment needs.
© 2021. The Author(s).
Conflict of interest statement
Two of the co-authors (DK and PDD) work in the public sector services in Sierra Leone. The other authors declare that they have no competing interests.
Figures
References
-
- The World Bank. Sierra Leone 2019. https://data.worldbank.org/country/sierra-leone. Accessed 20 Dec 2019.
-
- Lancet T. Ebola in West Africa: getting to zero. The Lancet. 2015;385(9968):578. - PubMed
-
- Musoke R, Chimbaru A, Jambai A, Njuguna C, Kayita J, Bunn J, et al. A Public health response to a mudslide in Freetown, Sierra Leone, 2017: Lessons Learnt. Disaster Med Public Health Prep. 2019;1:1–9. - PubMed
-
- Wai Z. Epistemologies of African conflicts: Violence, evolutionism, and the war in Sierra. Leone: Palgrave Macmillan; 2012.
-
- King's College London. King’s Centre for Global Health: About us 2015. https://www.kcl.ac.uk/lsm/research/divisions/global-health/about/index.aspx. Accessed 11 June 2015.]
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
