

Bacterial vaginosis: drivers of recurrence and challenges and opportunities in partner treatment
- PMID: 34470644
- PMCID: PMC8411528
- DOI: 10.1186/s12916-021-02077-3
Bacterial vaginosis: drivers of recurrence and challenges and opportunities in partner treatment
Abstract
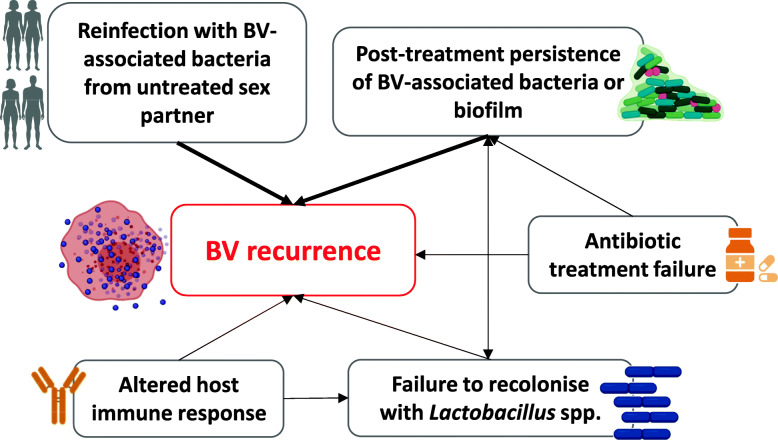
Bacterial vaginosis (BV) is the most common vaginal dysbiosis to affect women globally, yet an unacceptably high proportion of women experience BV recurrence within 6 months of recommended antibiotic therapy. The low rate of sustained cure highlights our limited understanding of the pathogenesis of BV recurrence, which has been attributed to possible persistence and re-emergence of BV-associated bacteria (BVAB) or a BV-associated biofilm following antimicrobials and/or reinfection occurring from sexual partners.There is a robust body of evidence to support the exchange of bacteria between partners during sexual activity, and while the hypothesis that women treated for BV are subsequently reinfected with BVAB following sex with an untreated sexual partner is not new, failure of past partner treatment trials has eroded confidence in this concept. If reinfection is a key driver of recurrence, current antimicrobial regimens directed to women alone are unlikely to achieve a high level of sustained cure, and the approach of partner treatment to reduce reinfection is justified. In this manuscript, we present the molecular and epidemiological evidence that underlies the hypothesis that BV is sexually transmitted, and summarise why research that continues to consider sexual partnerships is necessary. We also outline the significant barriers and challenges that we have identified while undertaking partner treatment studies, and we discuss the factors that impact on our ability to determine their effectiveness.Ultimately, the pathogenesis of BV recurrence is likely to be multifaceted and not attributable to a single mechanism in all women. If we are to achieve sustained cure for women, it is likely that combined and individualised approaches to eradicate BVAB, support an optimal vaginal microbiome, and prevent reinfection from partners will be required.
Keywords: Bacterial vaginosis; Clindamycin; Female partners; Male partners; Metronidazole; Penile microbiota; Sexually transmitted infection; Treatment; Urethral microbiota; Vaginal microbiota.
© 2021. The Author(s).
Conflict of interest statement
L.A.V. and C.S.B. receive funding from the Australian National Health and Medical Research Council for research pertaining to bacterial vaginosis. Melbourne Sexual Health Centre has received fees for advice on clinical trials on bacterial vaginosis, which is unrelated to this work. C.A.M is a consultant for Lupin Pharmaceuticals, BioFire Diagnostics, Cepheid, and PhagoMed. C.A.M has also received research funding support from Lupin Pharmaceuticals as well as speaker honoraria from Abbott Molecular, Cepheid, Roche Diagnostics, and Becton Dickinson. J.D.S has served as a consultant for Scynexis Pharmaceuticals and Mycovia Pharmaceutical.
Figures
References
-
- Brotman RM, Klebanoff MA, Nansel TR, Yu KF, Andrews WW, Zhang J, Schwebke JR. Bacterial vaginosis assessed by gram stain and diminished colonization resistance to incident gonococcal, chlamydial, and trichomonal genital infection. J Infect Dis. 2010;202(12):1907–1915. doi: 10.1086/657320. - DOI - PMC - PubMed
-
- Cohen CR, Lingappa JR, Baeten JM, Ngayo MO, Spiegel CA, Hong T, Donnell D, Celum C, Kapiga S, Delany S, Bukusi EA. Bacterial vaginosis associated with increased risk of female-to-male HIV-1 transmission: a prospective cohort analysis among African couples. PLoS Med. 2012;9(6):e1001251. doi: 10.1371/journal.pmed.1001251. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
