

Kidney Outcomes in Long COVID
- PMID: 34470828
- PMCID: PMC8806085
- DOI: 10.1681/ASN.2021060734
Kidney Outcomes in Long COVID
Abstract
Background: COVID-19 is associated with increased risk of post-acute sequelae involving pulmonary and extrapulmonary organ systems-referred to as long COVID. However, a detailed assessment of kidney outcomes in long COVID is not yet available.
Methods: We built a cohort of 1,726,683 US Veterans identified from March 1, 2020 to March 15, 2021, including 89,216 patients who were 30-day survivors of COVID-19 and 1,637,467 non-infected controls. We examined risks of AKI, eGFR decline, ESKD, and major adverse kidney events (MAKE). MAKE was defined as eGFR decline ≥50%, ESKD, or all-cause mortality. We used inverse probability-weighted survival regression, adjusting for predefined demographic and health characteristics, and algorithmically selected high-dimensional covariates, including diagnoses, medications, and laboratory tests. Linear mixed models characterized intra-individual eGFR trajectory.
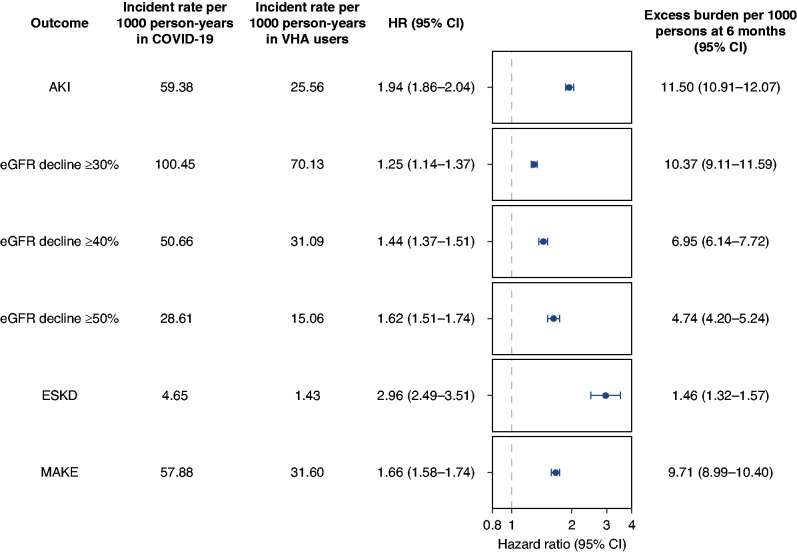
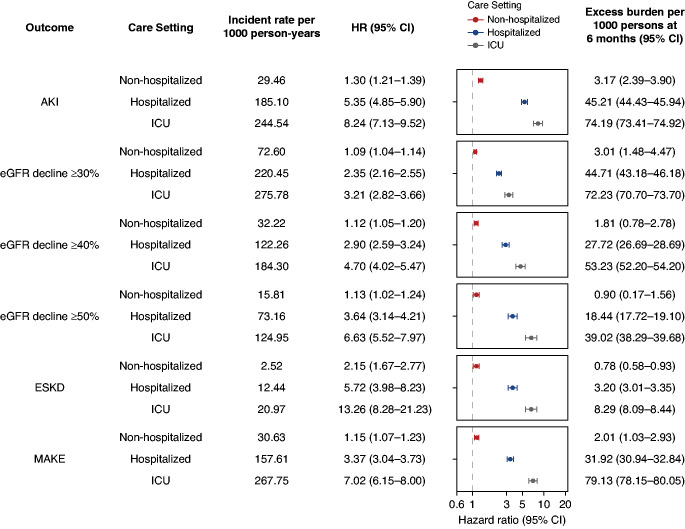
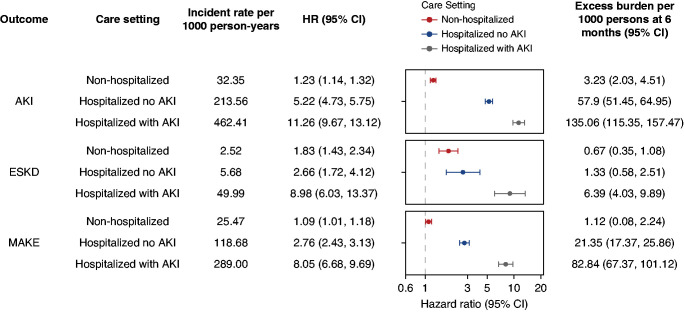
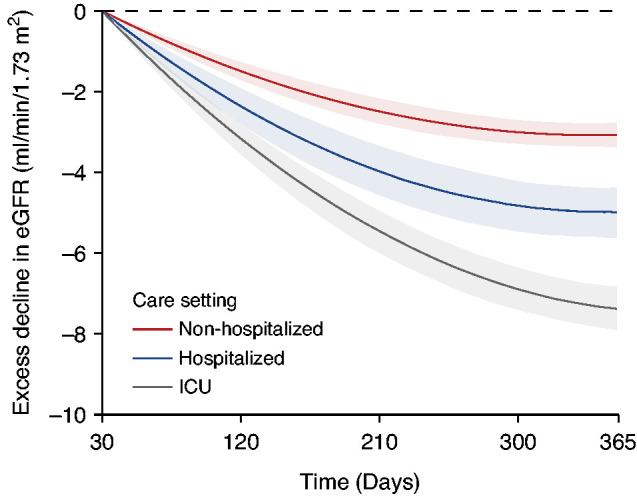
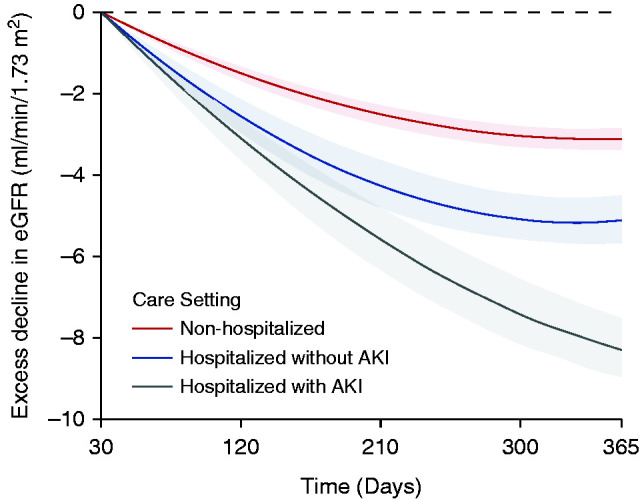
Results: Beyond the acute illness, 30-day survivors of COVID-19 exhibited a higher risk of AKI (aHR, 1.94; 95% CI, 1.86 to 2.04), eGFR decline ≥30% (aHR, 1.25; 95% CI, 1.14 to 1.37), eGFR decline ≥40% (aHR, 1.44; 95% CI, 1.37 to 1.51), eGFR decline ≥50% (aHR, 1.62; 95% CI, 1.51 to 1.74), ESKD (aHR, 2.96; 95% CI, 2.49 to 3.51), and MAKE (aHR, 1.66; 95% CI, 1.58 to 1.74). Increase in risks of post-acute kidney outcomes was graded according to the severity of the acute infection (whether patients were non-hospitalized, hospitalized, or admitted to intensive care). Compared with non-infected controls, 30-day survivors of COVID-19 exhibited excess eGFR decline (95% CI) of -3.26 (-3.58 to -2.94), -5.20 (-6.24 to -4.16), and -7.69 (-8.27 to -7.12) ml/min per 1.73 m2 per year, respectively, in non-hospitalized, hospitalized, and those admitted to intensive care during the acute phase of COVID-19 infection.
Conclusions: Patients who survived COVID-19 exhibited increased risk of kidney outcomes in the post-acute phase of the disease. Post-acute COVID-19 care should include attention to kidney disease.
Keywords: COVID-19; ESKD; ESRD; PASC; acute kidney injury; eGFR decline; kidney function; long COVID; post-acute COVID; post-acute sequelae of SARS-CoV-2 infection.
Copyright © 2021 by the American Society of Nephrology.
Figures
References
-
- Al-Aly Z, Xie Y, Bowe B: High-dimensional characterization of post-acute sequelae of COVID-19. Nature 594: 259–264, 2021 - PubMed
-
- Xie Y, Bowe B, Li T, Xian H, Yan Y, Al-Aly Z: Higher blood urea nitrogen is associated with increased risk of incident diabetes mellitus. Kidney Int 93: 741–752, 2018 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
