

Review Article: vaccination for patients with inflammatory bowel disease during the COVID-19 pandemic
- PMID: 34472643
- PMCID: PMC8653045
- DOI: 10.1111/apt.16590
Review Article: vaccination for patients with inflammatory bowel disease during the COVID-19 pandemic
Abstract
Background: Poor immune responses are frequently observed in patients with inflammatory bowel disease (IBD) receiving established vaccines; risk factors include immunosuppressants and active disease.
Aims: To summarise available information regarding immune responses achieved in patients with IBD receiving established vaccines. Using this information, to identify risk factors in the IBD population related to poor vaccine-induced immunity that may be applicable to vaccines against COVID-19.
Methods: We undertook a literature review on immunity to currently recommended vaccines for patients with IBD and to COVID-19 vaccines and summarised the relevant literature.
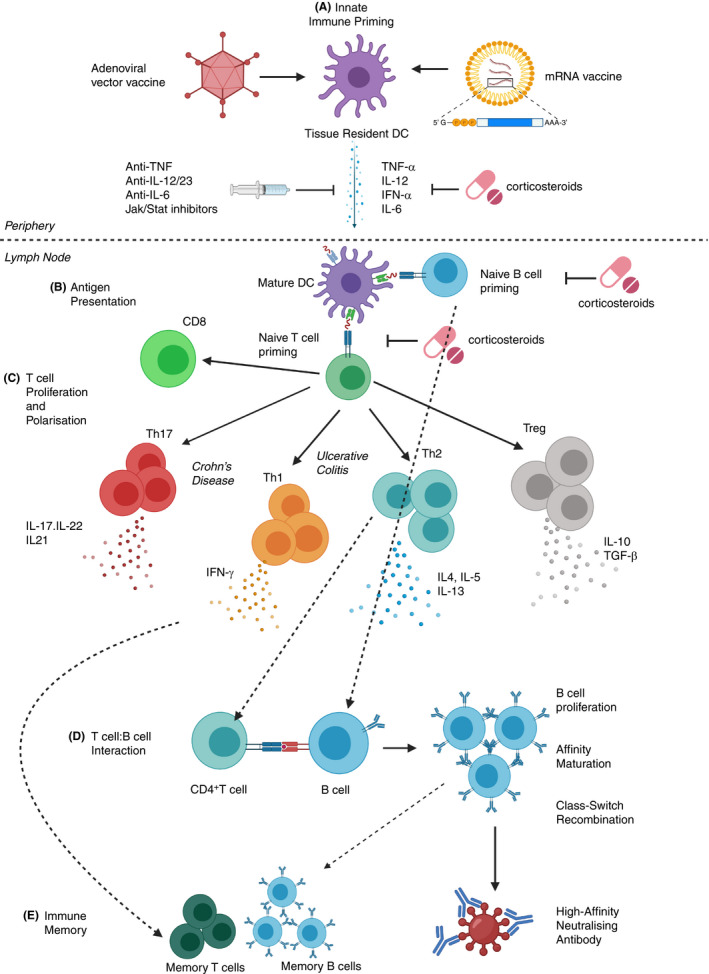
Results: Patients with IBD have reduced immune responses following vaccination compared to the general population. Factors including the use of immunomodulators and anti-TNF agents reduce response rates. Patients with IBD should be vaccinated against COVID-19 at the earliest opportunity as recommended by International Advisory Committees, and vaccination should not be deferred because a patient is receiving immune-modifying therapies. Antibody titres to COVID-19 vaccines appear to be reduced in patients receiving anti-TNF therapy, especially in combination with immunomodulators after one vaccination. Therefore, we should optimise any established risk factors that could impact response to vaccination in patients with IBD before vaccination.
Conclusions: Ideally, patients with IBD should be vaccinated at the earliest opportunity against COVID-19. Patients should be in remission and, if possible, have their corticosteroid dose minimised before vaccination. Further research is required to determine the impact of different biologics on vaccine response to COVID-19 and the potential for booster vaccines or heterologous prime-boost vaccinations in the IBD population.
© 2021 The Authors. Alimentary Pharmacology & Therapeutics published by John Wiley & Sons Ltd.
Figures
References
-
- Coronavirus disease (COVID‐19) – World Health Organization. World Health Organisation. 2021. https://www.who.int/emergencies/diseases/novel‐coronavirus‐2019. Accessed July 7, 2021.
-
- COVID‐19 and Your Health. Centres for Disease Control and Prevention. 2019. https://www.cdc.gov/coronavirus/2019‐ncov/need‐extra‐precautions/people‐.... Accessed January 3, 2021.
-
- Brenner EJ, Ungaro RC, Colombel JF & Kappelman MD. SECURE‐IBD Database Public Data Update. 2021. https://covidibd.org/current‐data/. Accessed July 7, 2021.
-
- Rahier Jf, Magro F, Abreu C, et al. Second European evidence‐based consensus on the prevention, diagnosis and management of opportunistic infections in inflammatory bowel disease. J Crohns Colitis. 2014;8:443‐468. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical