

Anticoagulation, therapy of concomitant conditions, and early rhythm control therapy: a detailed analysis of treatment patterns in the EAST - AFNET 4 trial
- PMID: 34473249
- PMCID: PMC8982435
- DOI: 10.1093/europace/euab200
Anticoagulation, therapy of concomitant conditions, and early rhythm control therapy: a detailed analysis of treatment patterns in the EAST - AFNET 4 trial
Erratum in
-
Corrigendum to: Anticoagulation, therapy of concomitant conditions, and early rhythm control therapy: a detailed analysis of treatment patterns in the EAST-AFNET 4 trial.Europace. 2022 Apr 5;24(4):564. doi: 10.1093/europace/euab277. Europace. 2022. PMID: 34897422 Free PMC article. No abstract available.
Abstract
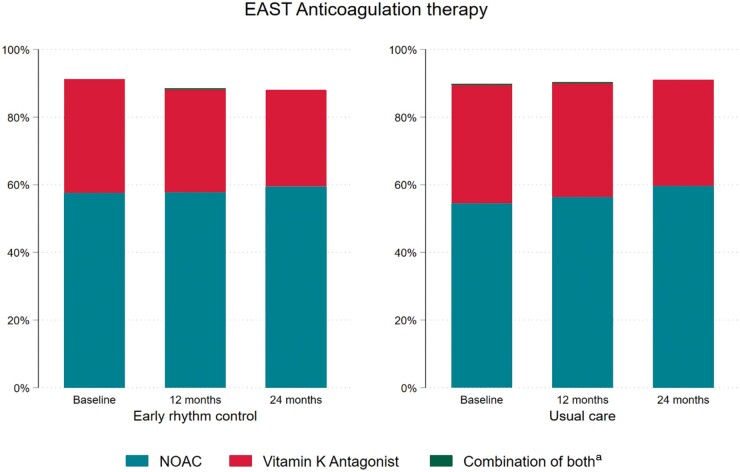
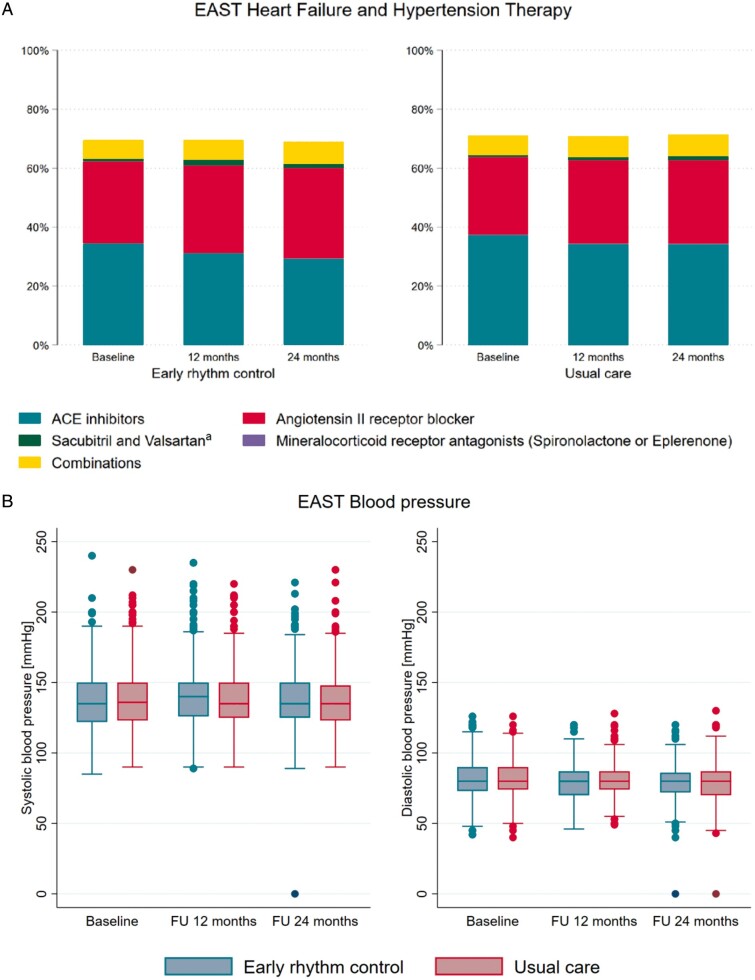
Aims: Treatment patterns were compared between randomized groups in EAST-AFNET 4 to assess whether differences in anticoagulation, therapy of concomitant diseases, or intensity of care can explain the clinical benefit achieved with early rhythm control in EAST-AFNET 4.
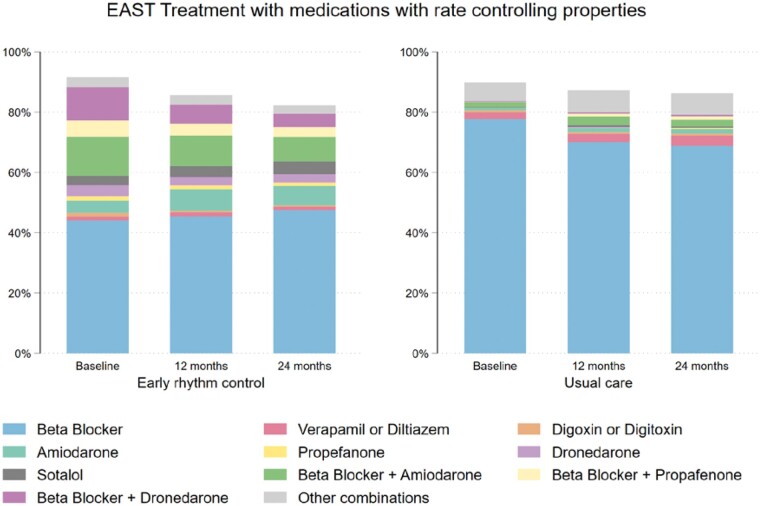
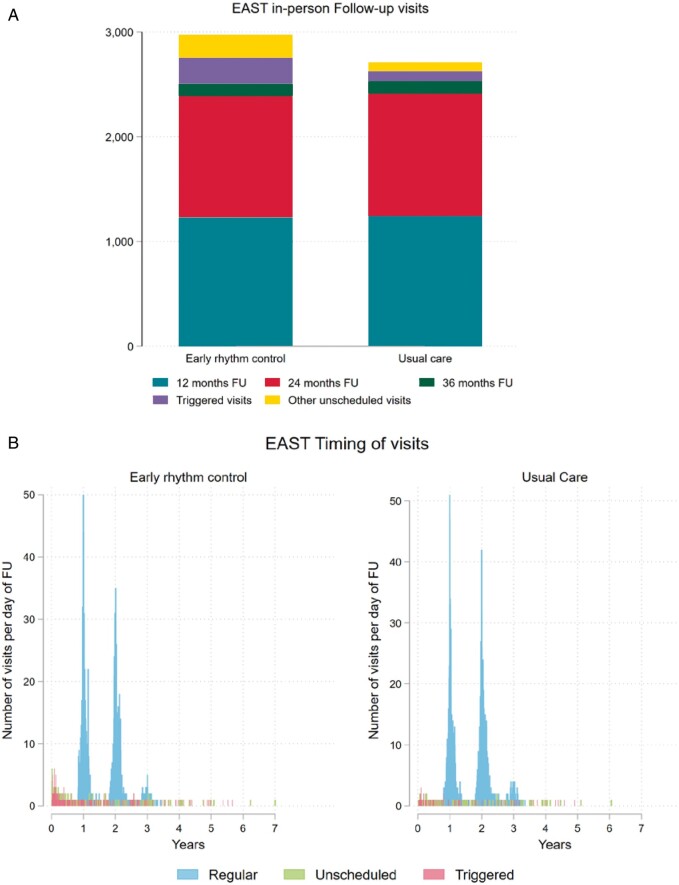
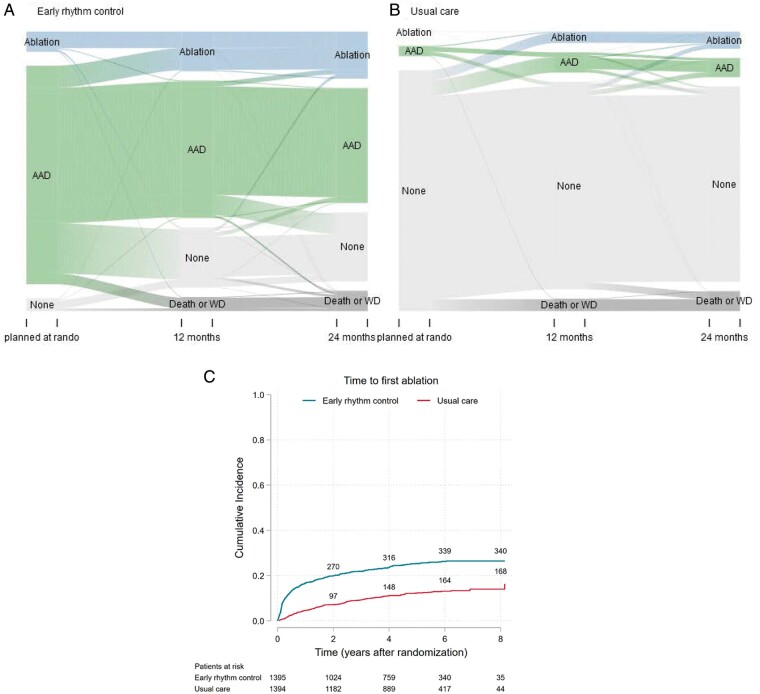
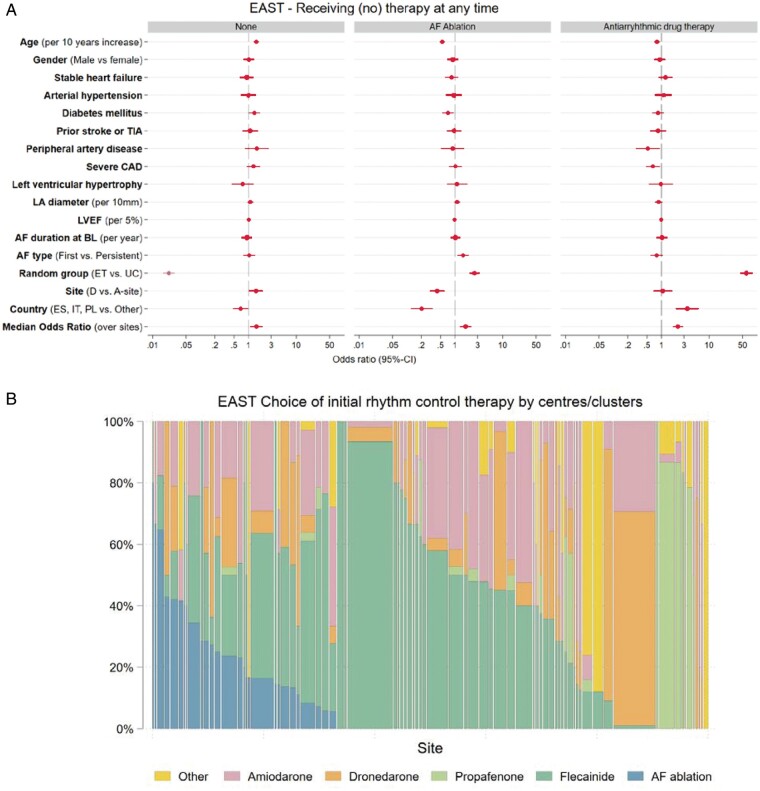
Methods and results: Cardiovascular treatment patterns and number of visits were compared between randomized groups in EAST-AFNET 4. Oral anticoagulation was used in >90% of patients during follow-up without differences between randomized groups. There were no differences in treatment of concomitant conditions between groups. The type of rhythm control varied by country and centre. Over time, antiarrhythmic drugs were given to 1171/1395 (84%) patients in early therapy, and to 202/1394 (14%) in usual care. Atrial fibrillation (AF) ablation was performed in 340/1395 (24%) patients randomized to early therapy, and in 168/1394 (12%) patients randomized to usual care. 97% of rhythm control therapies were within class I and class III recommendations of AF guidelines. Patients randomized to early therapy transmitted 297 166 telemetric electrocardiograms (ECGs) to a core lab. In total, 97 978 abnormal ECGs were sent to study sites. The resulting difference between study visits was low (0.06 visits/patient/year), with slightly more visits in early therapy (usual care 0.39 visits/patient/year; early rhythm control 0.45 visits/patient/year, P < 0.001), mainly due to visits for symptomatic AF recurrences or recurrent AF on telemetric ECGs.
Conclusion: The clinical benefit of early, systematic rhythm control therapy was achieved using variable treatment patterns of antiarrhythmic drugs and AF ablation, applied within guideline recommendations.
Keywords: Ablation; Antiarrhythmic drugs; Anticoagulation; Atrial fibrillation; Cardiovascular death; Heart failure; Rhythm control therapy; Stroke.
© The Author(s) 2021. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
References
-
- Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomstrom-Lundqvist C. et al.; ESC Scientific Document Group. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J 2021;42:373–498. - PubMed
-
- January CT, Wann LS, Calkins H, Chen LY, Cigarroa JE, Cleveland JC Jr. et al. 2019 AHA/ACC/HRS focused update of the 2014 AHA/ACC/HRS Guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society in Collaboration With the Society of Thoracic Surgeons. Circulation 2019;140:e125–51. - PubMed
-
- Packer DL, Mark DB, Robb RA, Monahan KH, Bahnson TD, Poole JE. et al.; for the CABANA Investigators. Effect of catheter ablation vs antiarrhythmic drug therapy on mortality, stroke, bleeding, and cardiac arrest among patients with atrial fibrillation: the CABANA randomized clinical trial. JAMA 2019;321:1261–74. - PMC - PubMed
-
- Marijon E, Le Heuzey JY, Connolly S, Yang S, Pogue J, Brueckmann M. et al. Causes of death and influencing factors in patients with atrial fibrillation: a competing-risk analysis from the randomized evaluation of long-term anticoagulant therapy study. Circulation 2013;128:2192–201. - PubMed
-
- Kotecha D, Breithardt G, Camm AJ, Lip GYH, Schotten U, Ahlsson A. et al. Integrating new approaches to atrial fibrillation management: the 6th AFNET/EHRA Consensus Conference. Europace 2018;20:395–407. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- PG/18/33/33780/BHF_/British Heart Foundation/United Kingdom
- Sanofi
- FS/13/43/30324/BHF_/British Heart Foundation/United Kingdom
- AA/18/2/34218/BHF_/British Heart Foundation/United Kingdom
- German Centre for Cardiovascular Research supported by the German Ministry of Education and Research (DZHK)
- AFNET, DZHK
- Abbott Laboratories
- Leducq Foundation
- EHRA, DHS
- NCT01288352/ClinicalTrials.gov
- PG/17/30/32961/BHF_/British Heart Foundation/United Kingdom
- German Ministry of Education and Research (DZHK), and Leducq Foundation
- ISRCTN04708680/EAST-AFNET 4 ISRCTN
- ISRCTN04708680/AFNET, DZHK, EHRA, DHS, Abbott Laboratories, Sanofi
- EU IMI 116074/European Union BigData@Heart
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
