

Evaluation of an Educational Outreach and Audit and Feedback Program to Reduce Continuous Pulse Oximetry Use in Hospitalized Infants With Stable Bronchiolitis: A Nonrandomized Clinical Trial
- PMID: 34473258
- PMCID: PMC8414187
- DOI: 10.1001/jamanetworkopen.2021.22826
Evaluation of an Educational Outreach and Audit and Feedback Program to Reduce Continuous Pulse Oximetry Use in Hospitalized Infants With Stable Bronchiolitis: A Nonrandomized Clinical Trial
Abstract
Importance: National guidelines recommend against continuous pulse oximetry use for hospitalized children with bronchiolitis who are not receiving supplemental oxygen, yet guideline-discordant use remains high.
Objectives: To evaluate deimplementation outcomes of educational outreach and audit and feedback strategies aiming to reduce guideline-discordant continuous pulse oximetry use in children hospitalized with bronchiolitis who are not receiving supplemental oxygen.
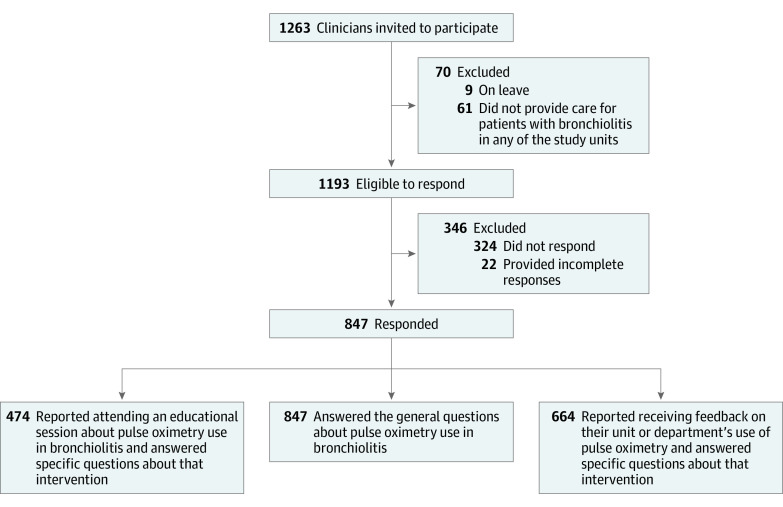
Design, setting, and participants: A nonrandomized clinical single-group deimplementation trial was conducted in 14 non-intensive care units in 5 freestanding children's hospitals and 1 community hospital from December 1, 2019, through March 14, 2020, among 847 nurses and physicians caring for hospitalized children with bronchiolitis who were not receiving supplemental oxygen.
Interventions: Educational outreach focused on communicating details of the existing guidelines and evidence. Audit and feedback strategies included 2 formats: (1) weekly aggregate data feedback to multidisciplinary teams with review of unit-level and hospital-level use of continuous pulse oximetry, and (2) real-time 1:1 feedback to clinicians when guideline-discordant continuous pulse oximetry use was discovered during in-person data audits.
Main outcomes and measures: Clinician ratings of acceptability, appropriateness, feasibility, and perceived safety were assessed using a questionnaire. Guideline-discordant continuous pulse oximetry use in hospitalized children was measured using direct observation of a convenience sample of patients with bronchiolitis who were not receiving supplemental oxygen.
Results: A total of 847 of 1193 eligible clinicians (695 women [82.1%]) responded to a Likert scale-based questionnaire (71% response rate). Most respondents rated the deimplementation strategies of education and audit and feedback as acceptable (education, 435 of 474 [92%]; audit and feedback, 615 of 664 [93%]), appropriate (education, 457 of 474 [96%]; audit and feedback, 622 of 664 [94%]), feasible (education, 424 of 474 [89%]; audit and feedback, 557 of 664 [84%]), and safe (803 of 847 [95%]). Sites collected 1051 audit observations (range, 47-403 per site) on 709 unique patient admissions (range, 31-251 per site) during a 3.5-month period of continuous pulse oximetry use in children with bronchiolitis not receiving supplemental oxygen, which were compared with 579 observations (range, 57-154 per site) from the same hospitals during the baseline 4-month period (prior season) to determine whether the strategies were associated with a reduction in use. Sites conducted 148 in-person educational outreach and aggregate data feedback sessions and provided real-time 1:1 feedback 171 of 236 times (72% of the time when guideline-discordant monitoring was identified). Adjusted for age, gestational age, time since weaning from supplemental oxygen, and other characteristics, guideline-discordant continuous pulse oximetry use decreased from 53% (95% CI, 49%-57%) to 23% (95% CI, 20%-25%) (P < .001) during the intervention period. There were no adverse events attributable to reduced monitoring.
Conclusions and relevance: In this nonrandomized clinical trial, educational outreach and audit and feedback deimplementation strategies for guideline-discordant continuous pulse oximetry use among hospitalized children with bronchiolitis who were not receiving supplemental oxygen were positively associated with clinician perceptions of feasibility, acceptability, appropriateness, and safety. Evaluating the sustainability of deimplementation beyond the intervention period is an essential next step.
Trial registration: ClinicalTrials.gov Identifier: NCT04178941.
Conflict of interest statement
Figures

Comment in
-
Deimplementing Continuous Pulse Oximetry in Patients With Bronchiolitis-What Are We Waiting For?JAMA Netw Open. 2021 Sep 1;4(9):e2123057. doi: 10.1001/jamanetworkopen.2021.23057. JAMA Netw Open. 2021. PMID: 34473263 No abstract available.
References
-
- Cunningham S, Rodriguez A, Adams T, et al. ; Bronchiolitis of Infancy Discharge Study (BIDS) group . Oxygen saturation targets in infants with bronchiolitis (BIDS): a double-blind, randomised, equivalence trial. Lancet. 2015;386(9998):1041-1048. doi:10.1016/S0140-6736(15)00163-4 - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
