

Physical Activity and Its Association with Traditional Outcome Measures in Pulmonary Arterial Hypertension
- PMID: 34473938
- PMCID: PMC8996274
- DOI: 10.1513/AnnalsATS.202105-560OC
Physical Activity and Its Association with Traditional Outcome Measures in Pulmonary Arterial Hypertension
Abstract
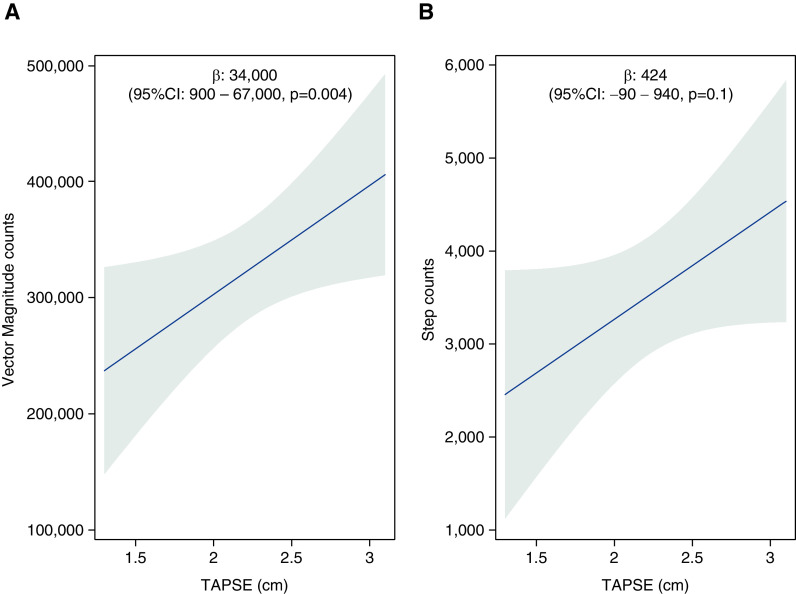
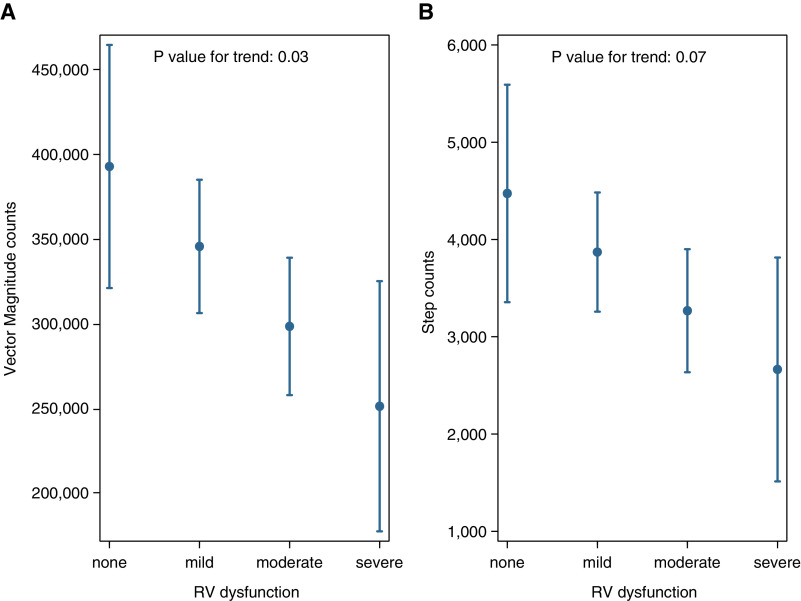
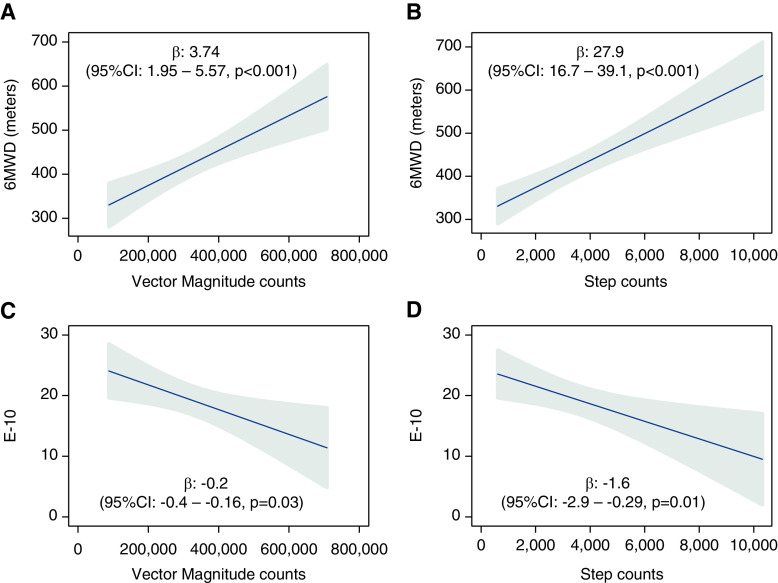
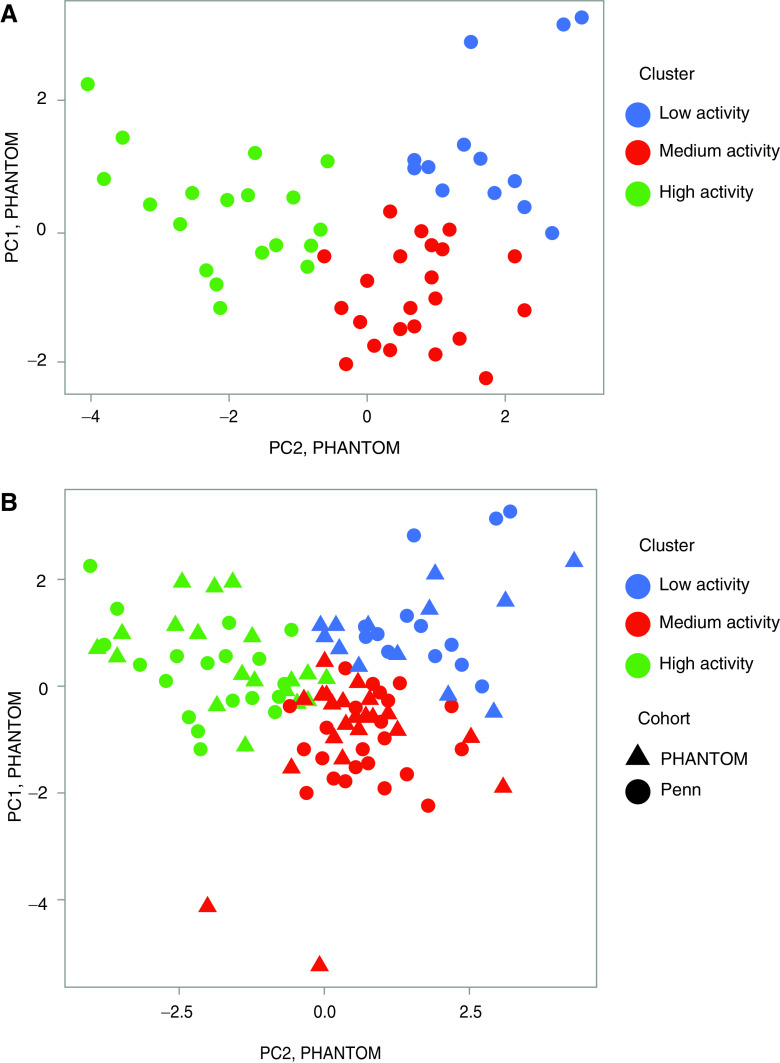
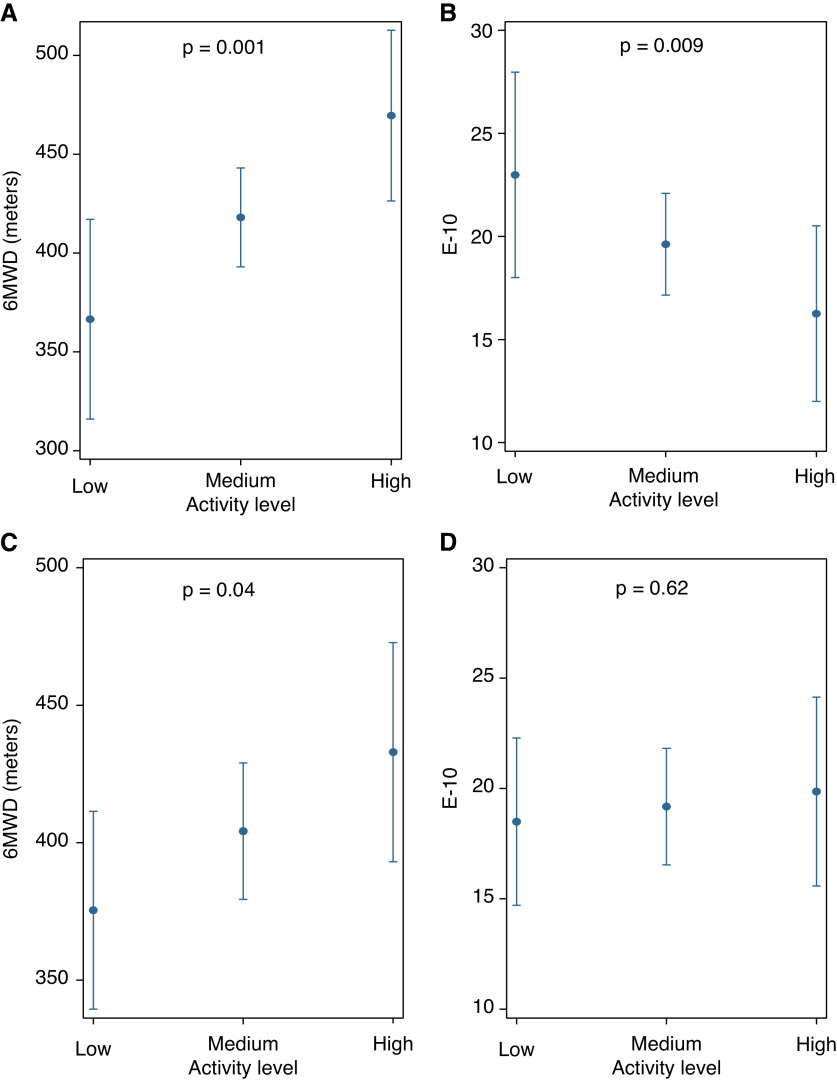
Rationale: Limitation of physical activity is a common presenting complaint for patients with pulmonary arterial hypertension (PAH). Physical activity is thought to be determined by cardiopulmonary function, yet there are limited data that investigate this relationship. Objectives: We aimed to study the relationship between right ventricular function and daily activity and its impact on health-related quality of life (HRQoL) in PAH. Methods: Baseline data for 55 patients enrolled in PHANTOM (Pulmonary Hypertension and Anastrozole), an ongoing multicenter randomized controlled trial of anastrozole in PAH, were used. Postmenopausal women and men were eligible and underwent 6-minute walk testing and echocardiography and completed HRQoL questionnaires. Each patient wore an accelerometer for 7 days. Multivariable linear regression models were used to study the association between tricuspid annular plane systolic excursion (TAPSE) and vector magnitude counts, and between daily activity and HRQoL. Principal component analysis and K-means clustering were used to identify activity-based phenotypes. K-nearest neighbors classification was applied to an independent cross-sectional cohort from the University of Pennsylvania. Results: The mean age of patients in PHANTOM was 61 years. In total, 67% were women with idiopathic PAH as the most common etiology. A 0.4-cm increase in TAPSE was associated with an increase in daily vector magnitude counts (β: 34,000; 95% confidence interval [CI], 900-67,000; P = 0.004) after adjustment for age, sex, body mass index, etiology of PAH, and wear time. A 1-SD increase in vector magnitude counts was associated with higher 6-minute walk distance (β: 56.1 m; 95% CI, 28.6-83.7; P < 0.001) and lower emPHasis-10 scores (β: -3.3; 95% CI, 0.3-6.4; P = 0.03). Three activity phenotypes, low, medium, and high, were identified. The most active phenotype had greater 6-minute walk distances (P = 0.001) and lower emPHasis-10 scores (P = 0.009) after adjustment for age, sex, body mass index, World Health Organization functional class, and parenteral prostacyclin use. Phenotypes of physical activity were reproduced in the second cohort and were independently associated with 6-minute walk distance. Conclusions: Better right ventricular systolic function was associated with increased levels of activity in PAH. Increased daily activity was associated with greater 6-minute walk distance and better HRQoL. Distinct activity-based phenotypes may be helpful in risk stratification of patients with PAH or provide novel endpoints for clinical trials.
Keywords: accelerometry; physical activity; pulmonary hypertension; quality of life.
Figures
References
-
- Galiè N, Humbert M, Vachiery JL, Gibbs S, Lang I, Torbicki A, et al. 2015 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT) Eur Respir J . 2015;46:903–975. - PubMed
-
- Haskell WL, Lee IM, Pate RR, Powell KE, Blair SN, Franklin BA, et al. Physical activity and public health: updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Med Sci Sports Exerc . 2007;39:1423–1434. - PubMed
-
- Seefeldt V, Malina RM, Clark MA. Factors affecting levels of physical activity in adults. Sports Med . 2002;32:143–168. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
