

Safety of Ocrelizumab in Patients With Relapsing and Primary Progressive Multiple Sclerosis
- PMID: 34475123
- PMCID: PMC8548959
- DOI: 10.1212/WNL.0000000000012700
Safety of Ocrelizumab in Patients With Relapsing and Primary Progressive Multiple Sclerosis
Abstract
Background and objectives: To report safety of ocrelizumab (OCR) up to 7 years in patients with relapsing multiple sclerosis (RMS) and primary progressive multiple sclerosis (PPMS) enrolled in clinical trials or treated in real-world postmarketing settings.
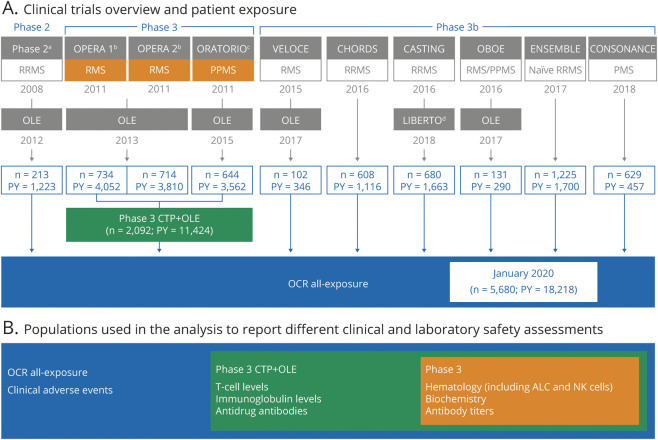
Methods: Safety analyses are based on integrated clinical and laboratory data for all patients who received OCR in 11 clinical trials, including the controlled treatment and open-label extension (OLE) periods of the phase 2 and 3 trials, plus the phase 3b trials VELOCE, CHORDS, CASTING, OBOE, ENSEMBLE, CONSONANCE, and LIBERTO. For selected adverse events (AEs), additional postmarketing data were used. Incidence rates of serious infections (SIs) and malignancies were contextualized using multiple epidemiologic sources.
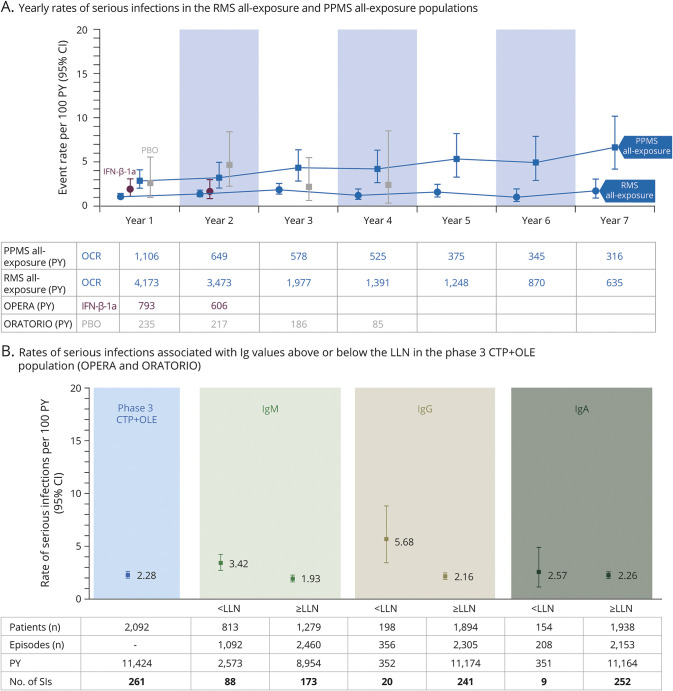
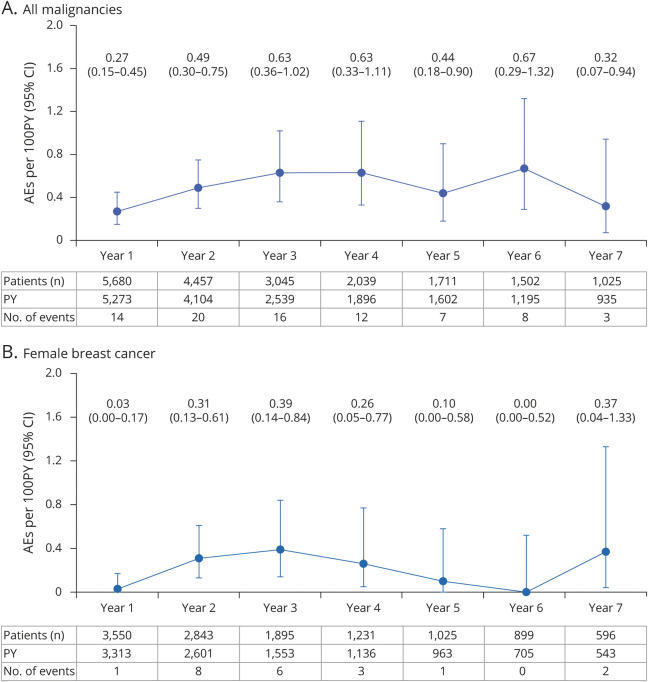
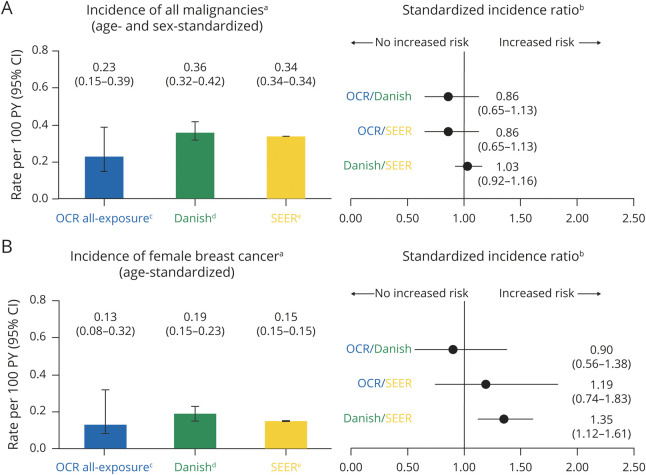
Results: At data cutoff (January 2020), 5,680 patients with multiple sclerosis (MS) received OCR (18,218 patient-years [PY] of exposure) in clinical trials. Rates per 100 PY (95% confidence interval) of AEs (248; 246-251), serious AEs (7.3; 7.0-7.7), infusion-related reactions (25.9; 25.1-26.6), and infections (76.2; 74.9-77.4) were similar to those within the controlled treatment period of the phase 3 trials. Rates of the most common serious AEs, including SIs (2.01; 1.81-2.23) and malignancies (0.46; 0.37-0.57), were consistent with the ranges reported in epidemiologic data.
Discussion: Continuous administration of OCR for up to 7 years in clinical trials, as well as its broader use for more than 3 years in the real-world setting, are associated with a favorable and manageable safety profile, without emerging safety concerns, in a heterogeneous MS population.
Classification of evidence: This analysis provides Class III evidence that long-term, continuous treatment with OCR has a consistent and favorable safety profile in patients with RMS and PPMS. This study is rated Class III because of the use of OLE data and historical controls.
Copyright © 2021 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Figures
Comment in
-
Longer-term Safety of B-Cell Therapy With Ocrelizumab in Multiple Sclerosis.Neurology. 2021 Oct 19;97(16):751-753. doi: 10.1212/WNL.0000000000012716. Epub 2021 Sep 2. Neurology. 2021. PMID: 34475129 No abstract available.
References
-
- DiLillo DJ, Hamaguchi Y, Ueda Y, et al. . Maintenance of long-lived plasma cells and serological memory despite mature and memory B cell depletion during CD20 immunotherapy in mice. J Immunol. 2008;180(1):361–371. - PubMed
-
- Kappos L, Li D, Calabresi PA, et al. . Ocrelizumab in relapsing-remitting multiple sclerosis: a phase 2, randomised, placebo-controlled, multicentre trial. Lancet. 2011;378(19805):1779–1787. - PubMed
-
- Hauser SL, Bar-Or A, Comi G, et al. . Ocrelizumab versus interferon beta-1a in relapsing multiple sclerosis. N Engl J Med. 2017;376:221–234. - PubMed
-
- Montalban X, Hauser SL, Kappos L, et al. . Ocrelizumab versus placebo in primary progressive multiple sclerosis. N Engl J Med. 2017;376(13):209–220. - PubMed