

Marfan syndrome
- PMID: 34475413
- PMCID: PMC9261969
- DOI: 10.1038/s41572-021-00298-7
Marfan syndrome
Erratum in
-
Publisher Correction: Marfan syndrome.Nat Rev Dis Primers. 2022 Jan 17;8(1):3. doi: 10.1038/s41572-022-00338-w. Nat Rev Dis Primers. 2022. PMID: 35039531 No abstract available.
Abstract
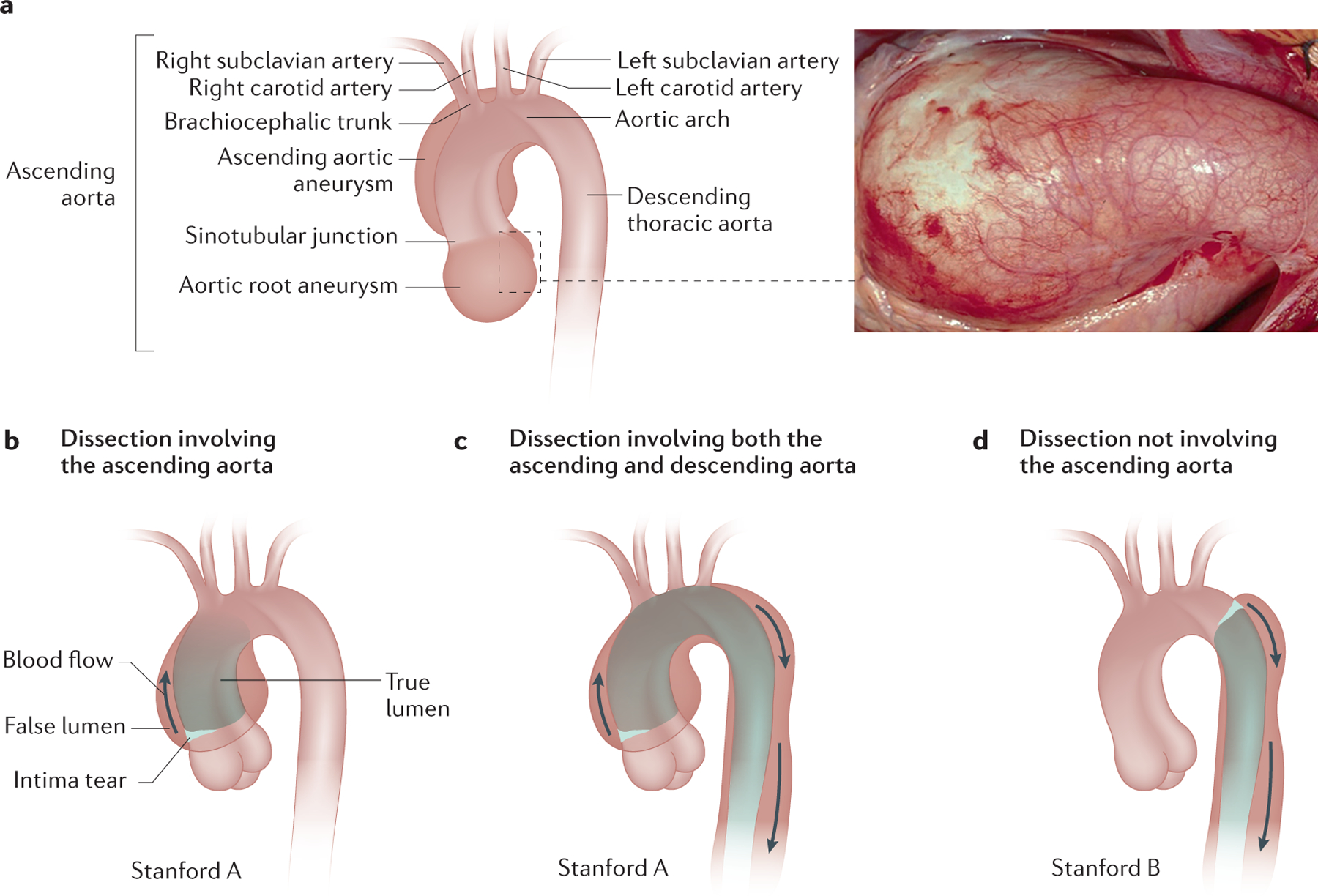
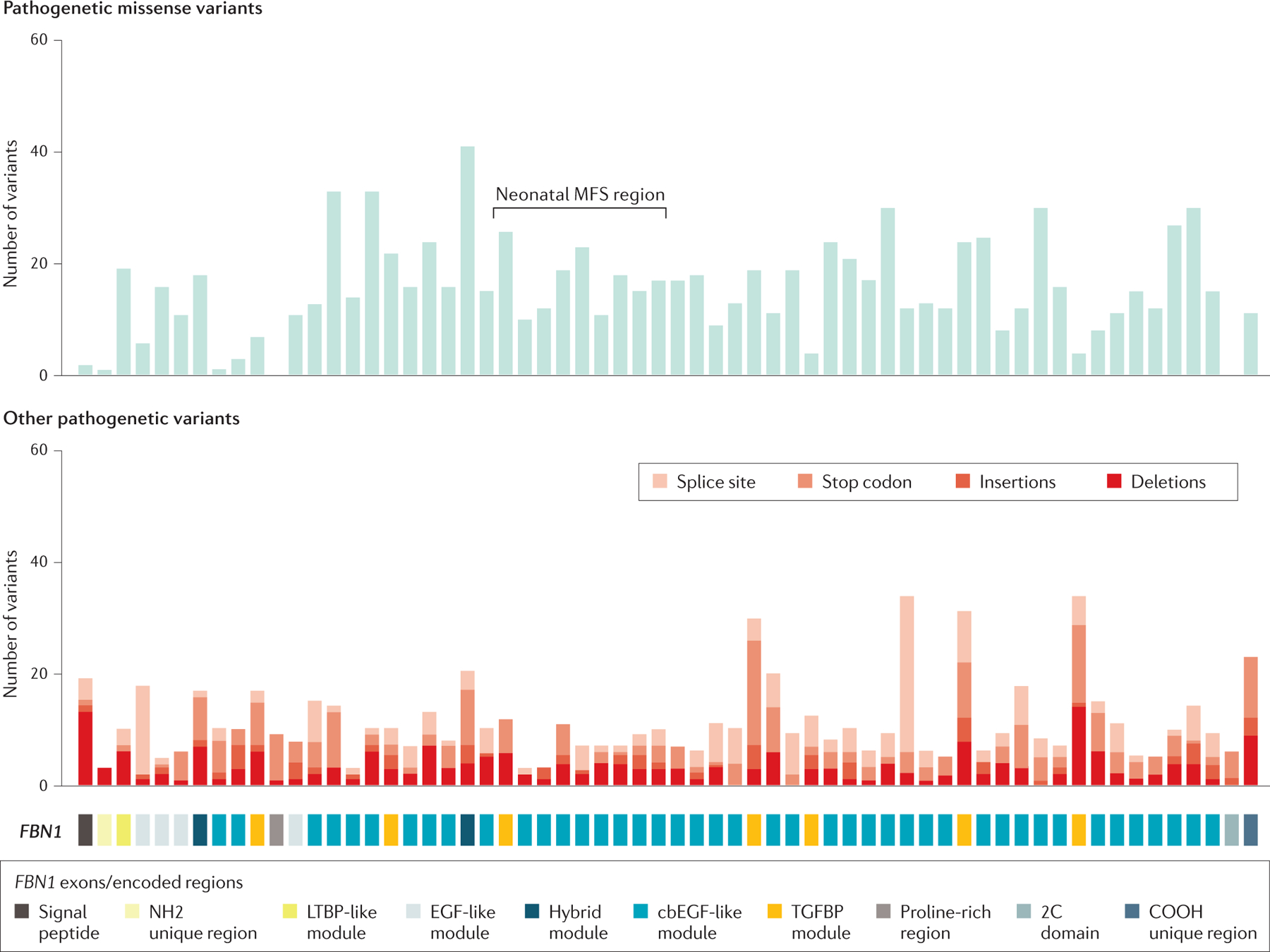
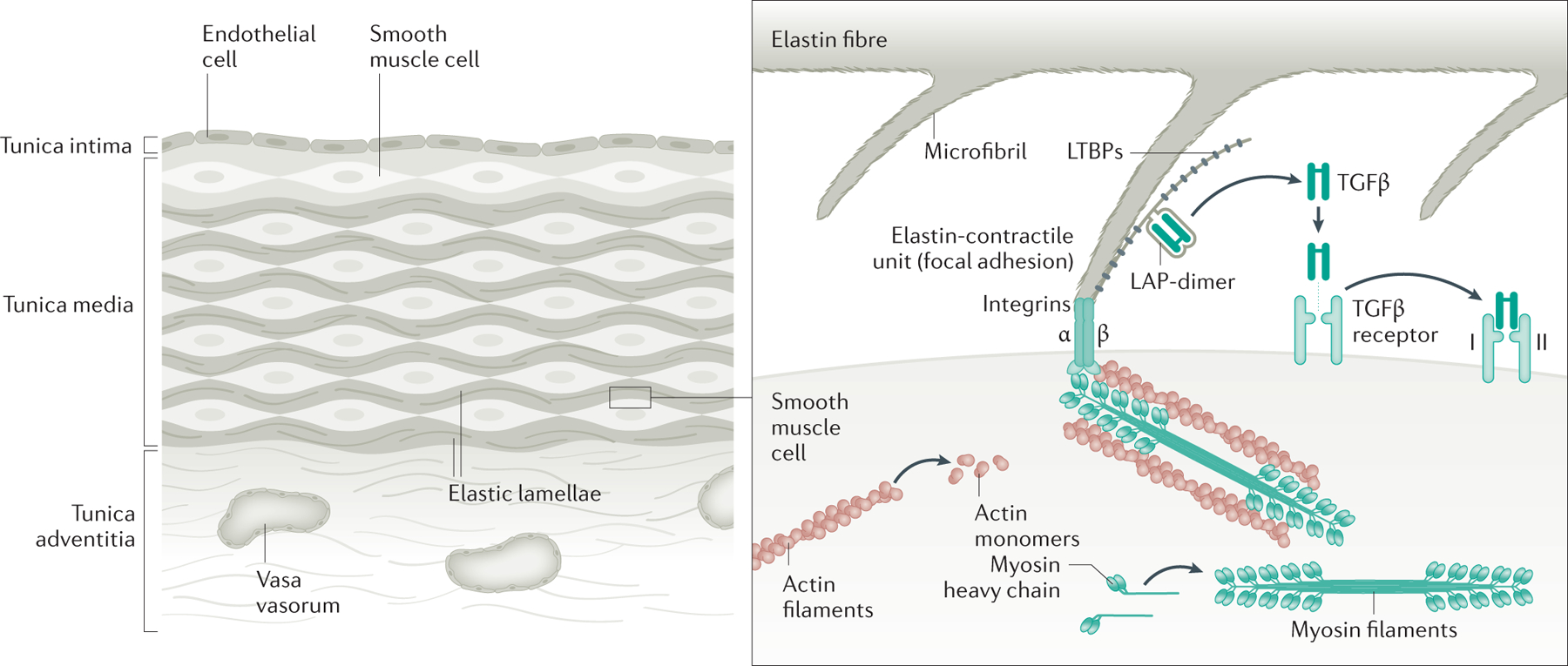
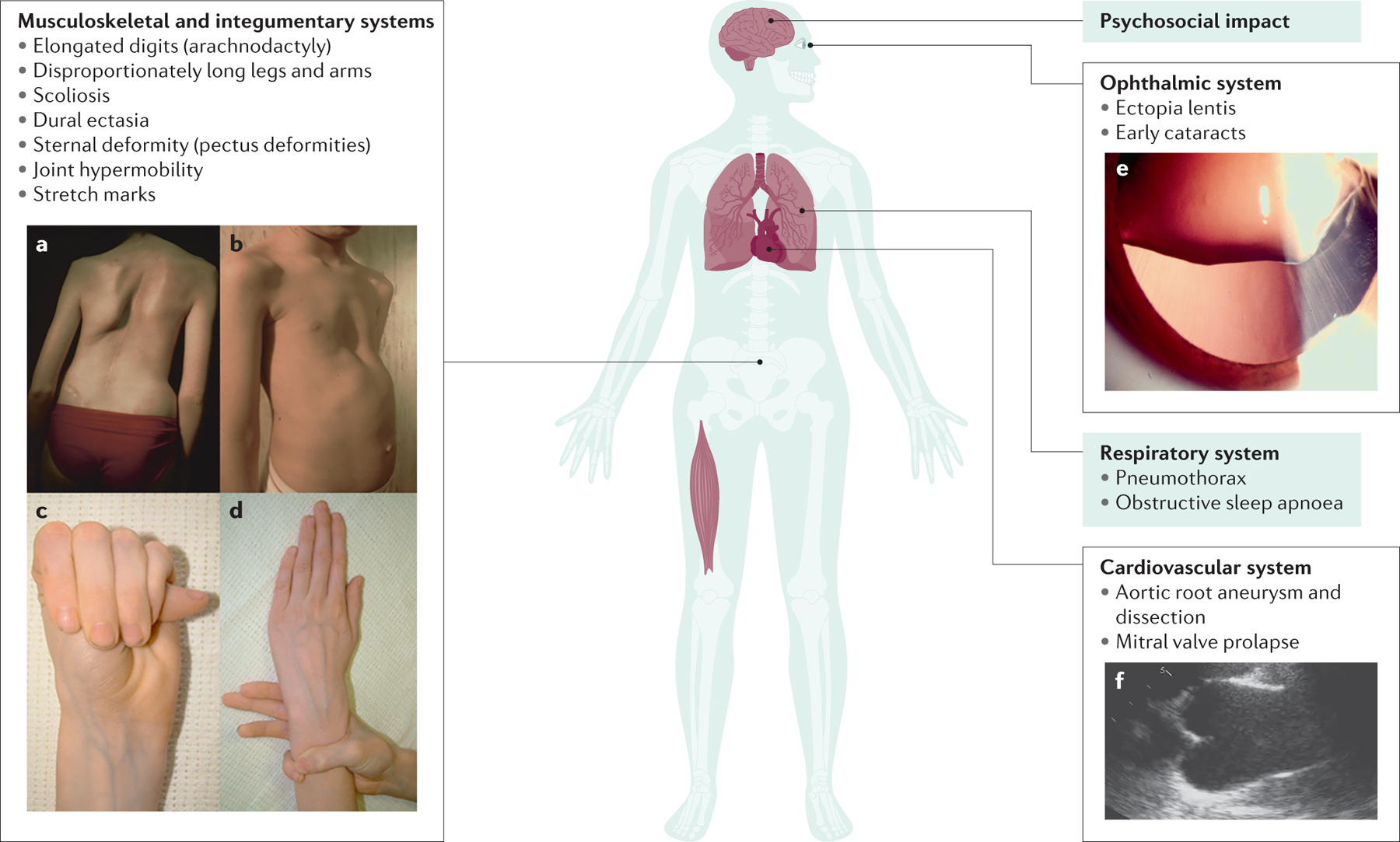
Marfan syndrome (MFS) is an autosomal dominant, age-related but highly penetrant condition with substantial intrafamilial and interfamilial variability. MFS is caused by pathogenetic variants in FBN1, which encodes fibrillin-1, a major structural component of the extracellular matrix that provides support to connective tissues, particularly in arteries, the pericondrium and structures in the eye. Up to 25% of individuals with MFS have de novo variants. The most prominent manifestations of MFS are asymptomatic aortic root aneurysms, aortic dissections, dislocation of the ocular lens (ectopia lentis) and skeletal abnormalities that are characterized by overgrowth of the long bones. MFS is diagnosed based on the Ghent II nosology; genetic testing confirming the presence of a FBN1 pathogenetic variant is not always required for diagnosis but can help distinguish MFS from other heritable thoracic aortic disease syndromes that can present with skeletal features similar to those in MFS. Untreated aortic root aneurysms can progress to life-threatening acute aortic dissections. Management of MFS requires medical therapy to slow the rate of growth of aneurysms and decrease the risk of dissection. Routine surveillance with imaging techniques such as transthoracic echocardiography, CT or MRI is necessary to monitor aneurysm growth and determine when to perform prophylactic repair surgery to prevent an acute aortic dissection.
© 2021. Springer Nature Limited.
Conflict of interest statement
Competing interest
The authors declare no competing interests
Figures
References
-
- Hollister DW, Godfrey M, Sakai LY & Pyeritz RE Immunohistologic abnormalities of the microfibrillar-fiber system in the Marfan syndrome. N. Engl. J. Med 323, 152–159 (1990). - PubMed
-
- Dietz HC et al. Marfan syndrome caused by a recurrent de novo missense mutation in the fibrillin gene. Nature 352, 337–339 (1991 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
