

A case of carotid endarterectomy assisted with a three-way junction shunting tube for the internal carotid artery stenosis involving a persistent primitive hypoglossal artery
- PMID: 34476076
- PMCID: PMC8407026
- DOI: 10.1093/jscr/rjab362
A case of carotid endarterectomy assisted with a three-way junction shunting tube for the internal carotid artery stenosis involving a persistent primitive hypoglossal artery
Abstract
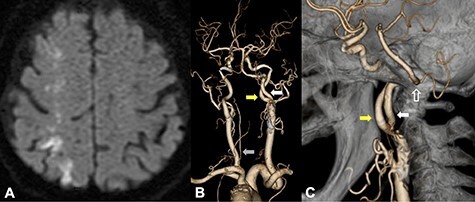
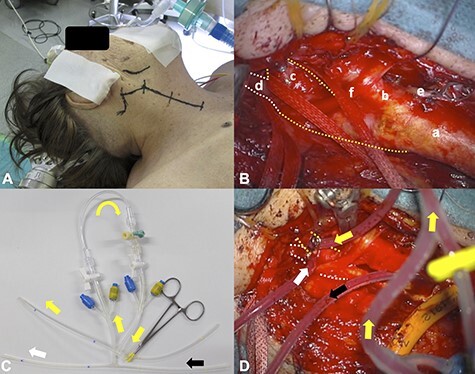
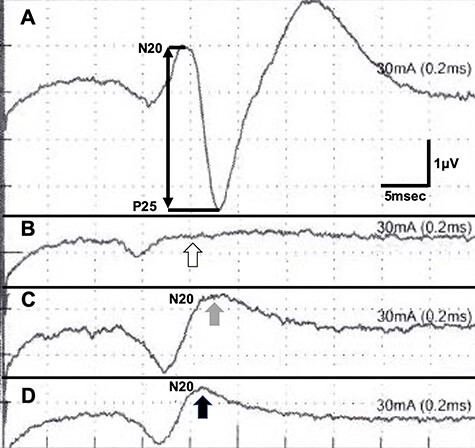
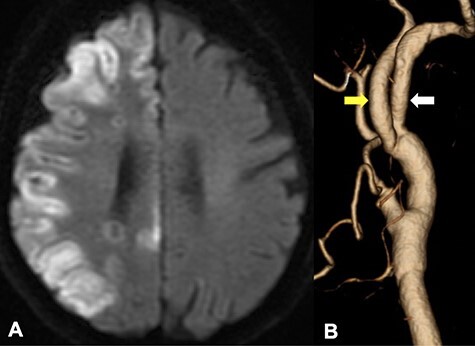
Only several cases of internal carotid artery (ICA) stenosis involving the persistent primitive hypoglossal artery (PPHA) have been treated with carotid endarterectomy (CEA) because of its extreme rarity. CEA was performed for an 87-year-old female with severe stenosis of the right ICA-PPHA bifurcation requiring shunting from CCA to both PPHA and ICA. We initially attempted to insert two intraluminal balloon shunts into the CCA, as previously reported. However, we found this procedure technically impossible to achieve. An improvised three-way junction tube was inserted distally into PPHA and ICA and proximally into CCA, securing blood flow during CEA. Unfortunately, the patient suffered post-operative ischemic brain lesions due to the prolonged ischemic time during our initial unsuccessful shunt attempt. A three-way junction shunting tube could be an effective shunt technique during an anatomically complicated CEA.
Keywords: carotid endarterectomy; endarterectomy; internal carotid artery stenosis; persistent primitive hypoglossal artery; shunt; three-way.
Published by Oxford University Press and JSCR Publishing Ltd. All rights reserved. © The Author(s) 2021.
Figures
References
-
- Zhang L, Song G, Chen L, Jiao L, Chen Y, Wang Y. Concomitant asymptomatic internal carotid artery and persistent primitive hypoglossal artery stenosis treated by endovascular stenting with proximal embolic protection. J Vasc Surg 2016;63:237–40. - PubMed
-
- Thomas JB, Antiga L, Che SL, Milner JS, Steinman DA, Spence JD, et al. Variation in the carotid bifurcation geometry of young versus older adults: implications for geometric risk of atherosclerosis. Stroke 2005;36:2450–6. - PubMed
-
- Thayer WP, Gaughen JR, Harthun NL. Surgical revascularization in the presence of a preserved primitive carotid-basilar communication. J Vasc Surg 2005;41:1066–9. - PubMed
-
- Megyesi JF, Findlay JM, Sherlock RA. Carotid endarterectomy in the presence of a persistent hypoglossal artery: case report. Neurosurgery 1997;41:669–72. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
