

Long-term follow-up including extensive complement analysis of a pediatric C3 glomerulopathy cohort
- PMID: 34476601
- PMCID: PMC8921070
- DOI: 10.1007/s00467-021-05221-6
Long-term follow-up including extensive complement analysis of a pediatric C3 glomerulopathy cohort
Abstract
Background: C3 glomerulopathy (C3G) is a rare kidney disorder characterized by predominant glomerular depositions of complement C3. C3G can be subdivided into dense deposit disease (DDD) and C3 glomerulonephritis (C3GN). This study describes the long-term follow-up with extensive complement analysis of 29 Dutch children with C3G.
Methods: Twenty-nine C3G patients (19 DDD, 10 C3GN) diagnosed between 1992 and 2014 were included. Clinical and laboratory findings were collected at presentation and during follow-up. Specialized assays were used to detect rare variants in complement genes and measure complement-directed autoantibodies and biomarkers in blood.
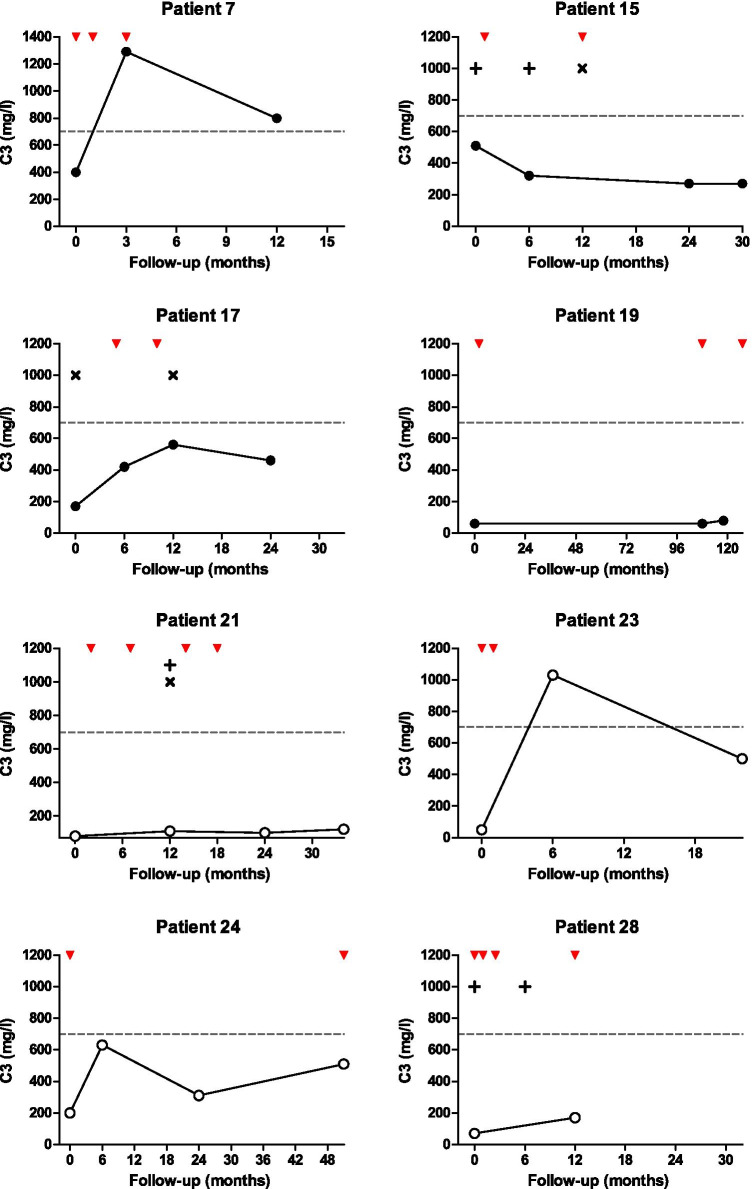
Results: DDD patients presented with lower estimated glomerular filtration rate (eGFR). C3 nephritic factors (C3NeFs) were detected in 20 patients and remained detectable over time despite immunosuppressive treatment. At presentation, low serum C3 levels were detected in 84% of all patients. During follow-up, in about 50% of patients, all of them C3NeF-positive, C3 levels remained low. Linear mixed model analysis showed that C3GN patients had higher soluble C5b-9 (sC5b-9) and lower properdin levels compared to DDD patients. With a median follow-up of 52 months, an overall benign outcome was observed with only six patients with eGFR below 90 ml/min/1.73 m2 at last follow-up.
Conclusions: We extensively described clinical and laboratory findings including complement features of an exclusively pediatric C3G cohort. Outcome was relatively benign, persistent low C3 correlated with C3NeF presence, and C3GN was associated with higher sC5b-9 and lower properdin levels. Prospective studies are needed to further elucidate the pathogenic mechanisms underlying C3G and guide personalized medicine with complement therapeutics.
Keywords: C3 glomerulonephritis; C3 glomerulopathy; C3 nephritic factor; Children; Complement system; Dense deposit disease.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Pickering MC, D'Agati VD, Nester CM, Smith RJ, Haas M, Appel GB, Alpers CE, Bajema IM, Bedrosian C, Braun M, Doyle M, Fakhouri F, Fervenza FC, Fogo AB, Fremeaux-Bacchi V, Gale DP, Goicoechea de Jorge E, Griffin G, Harris CL, Holers VM, Johnson S, Lavin PJ, Medjeral-Thomas N, Paul Morgan B, Nast CC, Noel LH, Peters DK, Rodriguez de Cordoba S, Servais A, Sethi S, Song WC, Tamburini P, Thurman JM, Zavros M, Cook HT. C3 glomerulopathy: consensus report. Kidney Int. 2013;84:1079–1089. doi: 10.1038/ki.2013.377. - DOI - PMC - PubMed
-
- Smith RJH, Appel GB, Blom AM, Cook HT, D'Agati VD, Fakhouri F, Fremeaux-Bacchi V, Jozsi M, Kavanagh D, Lambris JD, Noris M, Pickering MC, Remuzzi G, de Cordoba SR, Sethi S, Van der Vlag J, Zipfel PF, Nester CM. C3 glomerulopathy - understanding a rare complement-driven renal disease. Nat Rev Nephrol. 2019;15:129–143. doi: 10.1038/s41581-018-0107-2. - DOI - PMC - PubMed
-
- Servais A, Noel LH, Roumenina LT, Le Quintrec M, Ngo S, Dragon-Durey MA, Macher MA, Zuber J, Karras A, Provot F, Moulin B, Grunfeld JP, Niaudet P, Lesavre P, Fremeaux-Bacchi V. Acquired and genetic complement abnormalities play a critical role in dense deposit disease and other C3 glomerulopathies. Kidney Int. 2012;82:454–464. doi: 10.1038/ki.2012.63. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
