

Artificial intelligence-assisted colonoscopy: A prospective, multicenter, randomized controlled trial of polyp detection
- PMID: 34477306
- PMCID: PMC8525182
- DOI: 10.1002/cam4.4261
Artificial intelligence-assisted colonoscopy: A prospective, multicenter, randomized controlled trial of polyp detection
Abstract
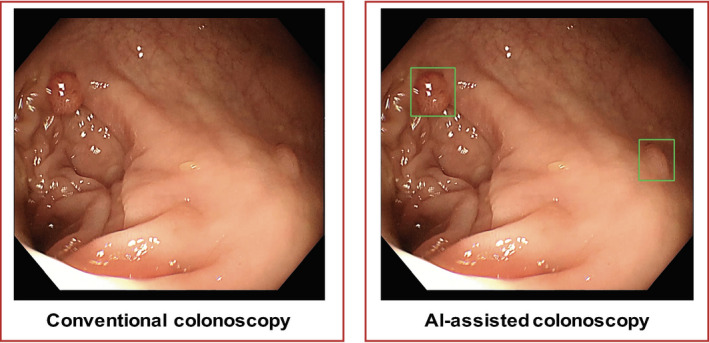
Background: Artificial intelligence (AI) assistance has been considered as a promising way to improve colonoscopic polyp detection, but there are limited prospective studies on real-time use of AI systems.
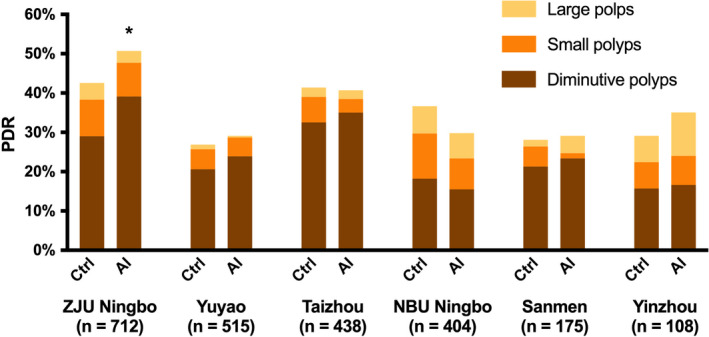
Methods: We conducted a prospective, multicenter, randomized controlled trial of patients undergoing colonoscopy at six centers. Eligible patients were randomly assigned to conventional colonoscopy (control group) or AI-assisted colonoscopy (AI group). AI assistance was our newly developed AI system for real-time colonoscopic polyp detection. Primary outcome is polyp detection rate (PDR). Secondary outcomes include polyps per positive patient (PPP), polyps per colonoscopy (PPC), and non-first polyps per colonoscopy (PPC-Plus).
Results: A total of 2352 patients were included in the final analysis. Compared with the control, AI group did not show significant increment in PDR (38.8% vs. 36.2%, p = 0.183), but its PPC-Plus was significantly higher (0.5 vs. 0.4, p < 0.05). In addition, AI group detected more diminutive polyps (76.0% vs. 68.8%, p < 0.01) and flat polyps (5.9% vs. 3.3%, p < 0.05). The effects varied somewhat between centers. In further logistic regression analysis, AI assistance independently contributed to the increment of PDR, and the impact was more pronounced for male endoscopists, shorter insertion time but longer withdrawal time, and elderly patients with larger waist circumference.
Conclusion: The intervention of AI plays a limited role in overall polyp detection, but increases detection of easily missed polyps; ChiCTR.org.cn number, ChiCTR1800015607.
Keywords: artificial intelligence; cancer prevention; colorectal polyps; endoscopy; image analysis.
© 2021 The Authors. Cancer Medicine published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures

Similar articles
-
Effect of artificial intelligence-aided colonoscopy for adenoma and polyp detection: a meta-analysis of randomized clinical trials.Int J Colorectal Dis. 2022 Mar;37(3):495-506. doi: 10.1007/s00384-021-04062-x. Epub 2021 Nov 11. Int J Colorectal Dis. 2022. PMID: 34762157 Review.
-
A prospective multicenter randomized controlled trial on artificial intelligence assisted colonoscopy for enhanced polyp detection.Sci Rep. 2024 Oct 26;14(1):25453. doi: 10.1038/s41598-024-77079-1. Sci Rep. 2024. PMID: 39455850 Free PMC article. Clinical Trial.
-
Artificial Intelligence-Assisted Colonoscopy for Colorectal Cancer Screening: A Multicenter Randomized Controlled Trial.Clin Gastroenterol Hepatol. 2023 Feb;21(2):337-346.e3. doi: 10.1016/j.cgh.2022.07.006. Epub 2022 Jul 19. Clin Gastroenterol Hepatol. 2023. PMID: 35863686
-
Use of a Novel Artificial Intelligence System Leads to the Detection of Significantly Higher Number of Adenomas During Screening and Surveillance Colonoscopy: Results From a Large, Prospective, US Multicenter, Randomized Clinical Trial.Am J Gastroenterol. 2024 Jul 1;119(7):1383-1391. doi: 10.14309/ajg.0000000000002664. Epub 2024 Jan 18. Am J Gastroenterol. 2024. PMID: 38235741 Clinical Trial.
-
Artificial Intelligence-Aided Colonoscopy for Polyp Detection: A Systematic Review and Meta-Analysis of Randomized Clinical Trials.J Laparoendosc Adv Surg Tech A. 2021 Oct;31(10):1143-1149. doi: 10.1089/lap.2020.0777. Epub 2021 Feb 1. J Laparoendosc Adv Surg Tech A. 2021. PMID: 33524298
Cited by
-
Randomised controlled trials evaluating artificial intelligence in clinical practice: a scoping review.Lancet Digit Health. 2024 May;6(5):e367-e373. doi: 10.1016/S2589-7500(24)00047-5. Lancet Digit Health. 2024. PMID: 38670745 Free PMC article.
-
The Impact of Computer-aided Detection Technology in Adenoma Detection Rate Among Experienced Endoscopists in the Community Setting.J Community Hosp Intern Med Perspect. 2024 Sep 9;14(5):42-48. doi: 10.55729/2000-9666.1396. eCollection 2024. J Community Hosp Intern Med Perspect. 2024. PMID: 39399190 Free PMC article.
-
Effectiveness of switching endoscopists for repeat surveillance colonoscopy: a retrospective study.BMC Gastroenterol. 2023 Oct 6;23(1):347. doi: 10.1186/s12876-023-02981-3. BMC Gastroenterol. 2023. PMID: 37803276 Free PMC article.
-
Artificial intelligence for colorectal neoplasia detection during colonoscopy: a systematic review and meta-analysis of randomized clinical trials.EClinicalMedicine. 2023 Nov 30;66:102341. doi: 10.1016/j.eclinm.2023.102341. eCollection 2023 Dec. EClinicalMedicine. 2023. PMID: 38078195 Free PMC article.
-
Requirement of image standardization for AI-based macroscopic diagnosis for surgical specimens of gastric cancer.J Cancer Res Clin Oncol. 2023 Aug;149(9):6467-6477. doi: 10.1007/s00432-022-04570-5. Epub 2023 Feb 11. J Cancer Res Clin Oncol. 2023. PMID: 36773090 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
