

Effects of Antiplatelet Therapy After Stroke Caused by Intracerebral Hemorrhage: Extended Follow-up of the RESTART Randomized Clinical Trial
- PMID: 34477823
- PMCID: PMC8417806
- DOI: 10.1001/jamaneurol.2021.2956
Effects of Antiplatelet Therapy After Stroke Caused by Intracerebral Hemorrhage: Extended Follow-up of the RESTART Randomized Clinical Trial
Abstract
Importance: The Restart or Stop Antithrombotics Randomized Trial (RESTART) found that antiplatelet therapy appeared to be safe up to 5 years after intracerebral hemorrhage (ICH) that had occurred during antithrombotic (antiplatelet or anticoagulant) therapy.
Objectives: To monitor adherence, increase duration of follow-up, and improve precision of estimates of the effects of antiplatelet therapy on recurrent ICH and major vascular events.
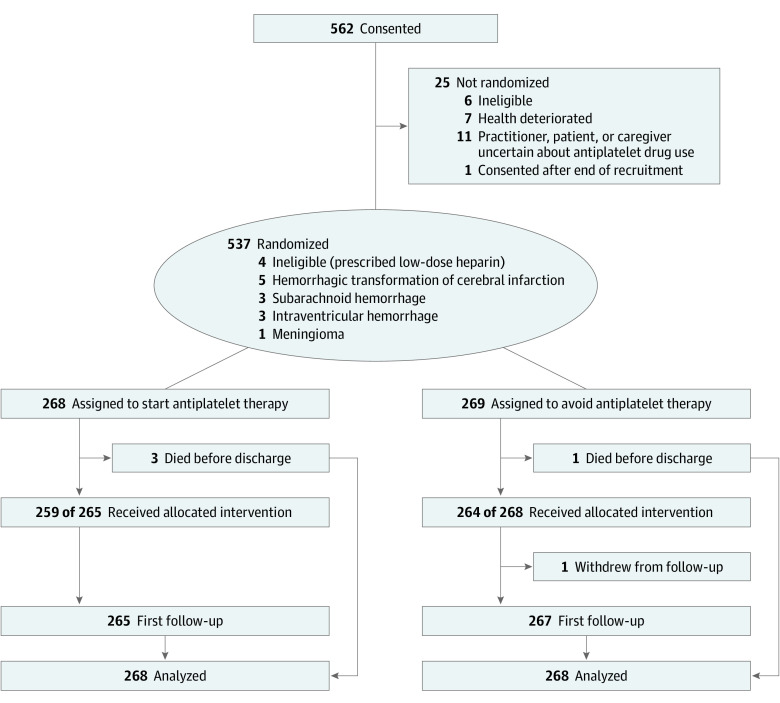
Design, setting and participants: From May 22, 2013, through May 31, 2018, this prospective, open, blinded end point, parallel-group randomized clinical trial studied 537 participants at 122 hospitals in the UK. Participants were individuals 18 years or older who had taken antithrombotic therapy for the prevention of occlusive vascular disease when they developed ICH, discontinued antithrombotic therapy, and survived for 24 hours. After initial follow-up ended on November 30, 2018, annual follow-up was extended until November 30, 2020, for a median of 3.0 years (interquartile range [IQR], 2.0-5.0 years) for the trial cohort.
Interventions: Computerized randomization that incorporated minimization allocated participants (1:1) to start or avoid antiplatelet therapy.
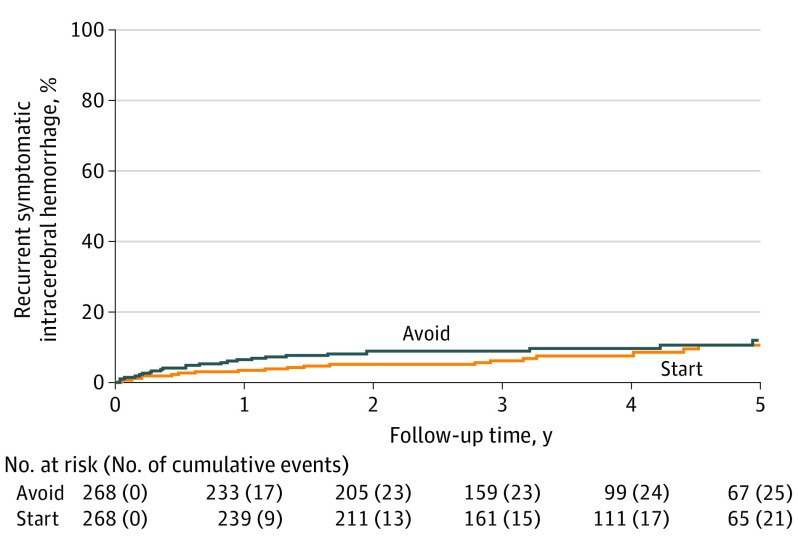
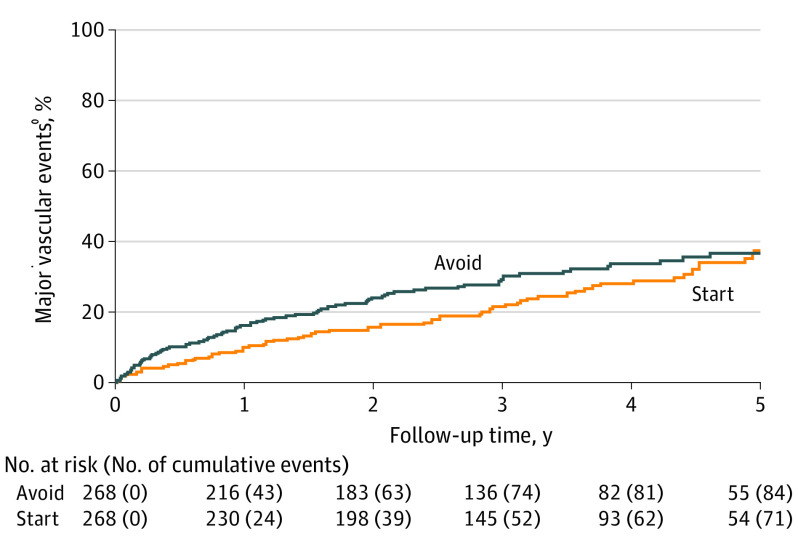
Main outcomes and measures: Participants were followed up for the primary outcome (recurrent symptomatic ICH) and secondary outcomes (all major vascular events) for up to 7 years. Data from all randomized participants were analyzed using Cox proportional hazards regression, adjusted for minimization covariates.
Results: A total of 537 patients (median age, 76.0 years; IQR, 69.0-82.0 years; 360 [67.0%] male; median time after ICH onset, 76.0 days; IQR, 29.0-146.0 days) were randomly allocated to start (n = 268) or avoid (n = 269 [1 withdrew]) antiplatelet therapy. The primary outcome of recurrent ICH affected 22 of 268 participants (8.2%) allocated to antiplatelet therapy compared with 25 of 268 participants (9.3%) allocated to avoid antiplatelet therapy (adjusted hazard ratio, 0.87; 95% CI, 0.49-1.55; P = .64). A major vascular event affected 72 participants (26.8%) allocated to antiplatelet therapy compared with 87 participants (32.5%) allocated to avoid antiplatelet therapy (hazard ratio, 0.79; 95% CI, 0.58-1.08; P = .14).
Conclusions and relevance: Among patients with ICH who had previously taken antithrombotic therapy, this study found no statistically significant effect of antiplatelet therapy on recurrent ICH or all major vascular events. These findings provide physicians with some reassurance about the use of antiplatelet therapy after ICH if indicated for secondary prevention of major vascular events.
Trial registration: isrctn.org Identifier: ISRCTN71907627.
Conflict of interest statement
Figures
Comment in
-
Blutverdünnung: Neustart nach Hirnblutung.MMW Fortschr Med. 2022 Sep;164(16):30-31. doi: 10.1007/s15006-022-1929-1. MMW Fortschr Med. 2022. PMID: 36123473 Review. German. No abstract available.
References
-
- O’Donnell MJ, Chin SL, Rangarajan S, et al. ; INTERSTROKE investigators . Global and regional effects of potentially modifiable risk factors associated with acute stroke in 32 countries (INTERSTROKE): a case-control study. Lancet. 2016;388(10046):761-775. doi:10.1016/S0140-6736(16)30506-2 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
