

Diagnostic Pitfalls in Cushing Disease: Surgical Remission Rates, Test Thresholds, and Lessons Learned in 105 Patients
- PMID: 34478542
- PMCID: PMC8684536
- DOI: 10.1210/clinem/dgab659
Diagnostic Pitfalls in Cushing Disease: Surgical Remission Rates, Test Thresholds, and Lessons Learned in 105 Patients
Abstract
Context: Confirming a diagnosis of Cushing disease (CD) remains challenging, yet is critically important before recommending transsphenoidal surgery for adenoma resection.
Objective: To describe predictive performance of preoperative biochemical and imaging data relative to post-operative remission and clinical characteristics in patients with presumed CD.
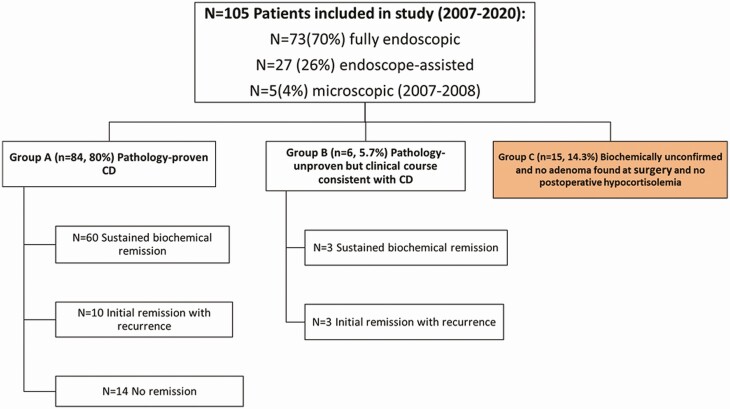
Design, setting, patients, interventions: Patients (n = 105; 86% female) who underwent surgery from 2007 through 2020 were classified into 3 groups: group A (n = 84) pathology-proven ACTH adenoma; group B (n = 6) pathology-unproven but with postoperative hypocortisolemia consistent with CD; and group C (n = 15) pathology-unproven, without postoperative hypocortisolemia. Group A + B were combined as confirmed CD and group C as unconfirmed CD.
Main outcomes: Group A + B was compared with group C regarding predictive performance of preoperative 24-hour urinary free cortisol (UFC), late night salivary cortisol (LNSC), 1-mg dexamethasone suppression test (DST), plasma ACTH, and pituitary magnetic resonance imaging (MRI).
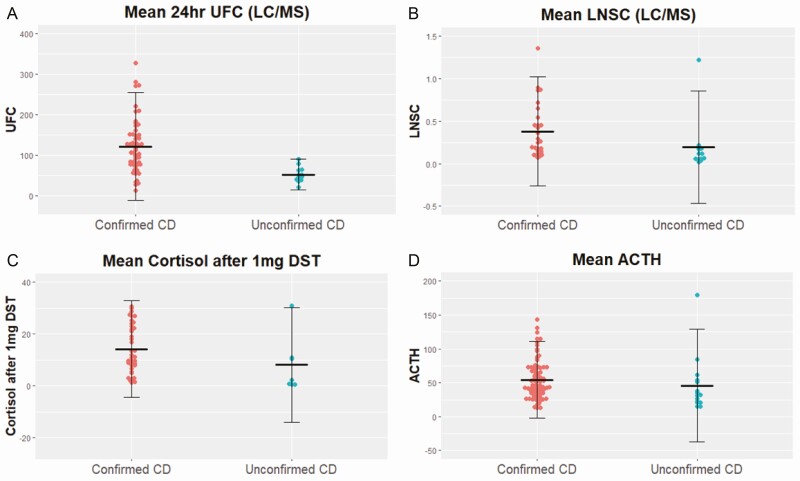
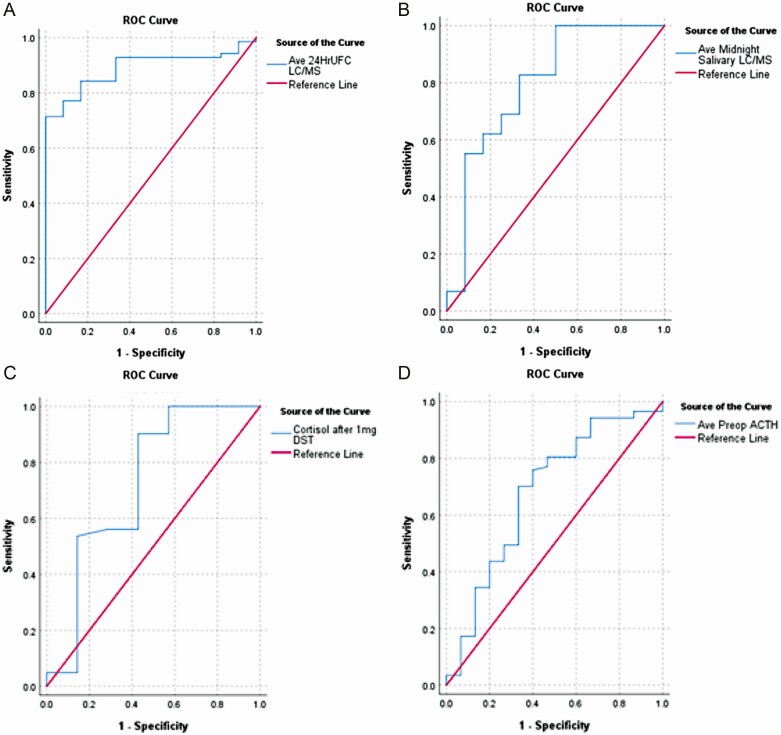
Results: All groups had a similar clinical phenotype. Compared with group C, group A + B had higher mean UFC (P < 0.001), LNSC (P = 0.003), DST (P = 0.06), and ACTH (P = 0.03) and larger MRI-defined lesions (P < 0.001). The highest accuracy thresholds were: UFC 72 µg/24 hours; LNSC 0.122 µg/dL, DST 2.70 µg/dL, and ACTH 39.1 pg/mL. Early (3-month) biochemical remission was achieved in 76/105 (72%) patients: 76/90(84%) and 0/15(0%) of group A + B vs group C, respectively, P < 0.0001. In group A + B, nonremission was strongly associated with adenoma cavernous sinus invasion.
Conclusions: Use of strict biochemical thresholds may help avoid offering transsphenoidal surgery to presumed CD patients with equivocal data and improve surgical remission rates. Patients with Cushingoid phenotype but equivocal biochemical data warrant additional rigorous testing.
Keywords: 24-hour urinary free cortisol; ACTH; Cushing’s disease; pituitary adenoma; salivary cortisol; transsphenoidal surgery.
© The Author(s) 2021. Published by Oxford University Press on behalf of the Endocrine Society.
Figures
Comment in
-
Polygenic risk score: a tool ready for clinical use?Eur Heart J. 2022 May 7;43(18):1712-1714. doi: 10.1093/eurheartj/ehab923. Eur Heart J. 2022. PMID: 35211747 No abstract available.
References
-
- Sharma ST; AACE Adrenal Scientific Committee . An individualized approach to the evaluation of cushing syndrome. Endocr Pract. 2017;23(6):726-737. - PubMed
-
- Wengander S, Trimpou P, Papakokkinou E, Ragnarsson O. The incidence of endogenous Cushing’s syndrome in the modern era. Clin Endocrinol. 2019;91(2):263-270. - PubMed
-
- Kreitschmann-Andermahr I, Psaras T, Tsiogka M, et al. . From first symptoms to final diagnosis of Cushing’s disease: experiences of 176 patients. Eur J Endocrinol. 2015;172(3):285-289. - PubMed
-
- Kelly DF. Transsphenoidal surgery for Cushing’s disease: a review of success rates, remission predictors, management of failed surgery, and Nelson’s Syndrome. Neurosurg Focus. 2007;23(3):E5. - PubMed
-
- Dallapiazza RF, Oldfield EH, Jane JA Jr. Surgical management of Cushing’s disease. Pituitary. 2015;18(2):211-216. - PubMed
