

Clinical characteristics and risk factors associated with Pneumocystis jirovecii infection in patients with solid tumors: study of thirteen-year medical records of a large cancer center
- PMID: 34479519
- PMCID: PMC8418024
- DOI: 10.1186/s12885-021-08727-2
Clinical characteristics and risk factors associated with Pneumocystis jirovecii infection in patients with solid tumors: study of thirteen-year medical records of a large cancer center
Abstract
Background: Pneumocystis jirovecii pneumonia (PCP)-related risk factors among patients with solid tumors are not completely defined. Thus, we aimed to characterize PCP cases with underlying solid tumors, to highlight the factors contributing to its development besides the prolonged use of moderate-to-high dose corticosteroids.
Methods: We retrospectively reviewed the medical records of patients with solid tumors diagnosed with PCP between 2006 and 2018 at a cancer center in Tokyo, Japan. Demographic and clinical data were collected, which included malignancy types, total lymphocyte count, coexisting pulmonary disease, chemotherapy, radiation therapy, corticosteroid use, and PCP-attributable mortality.
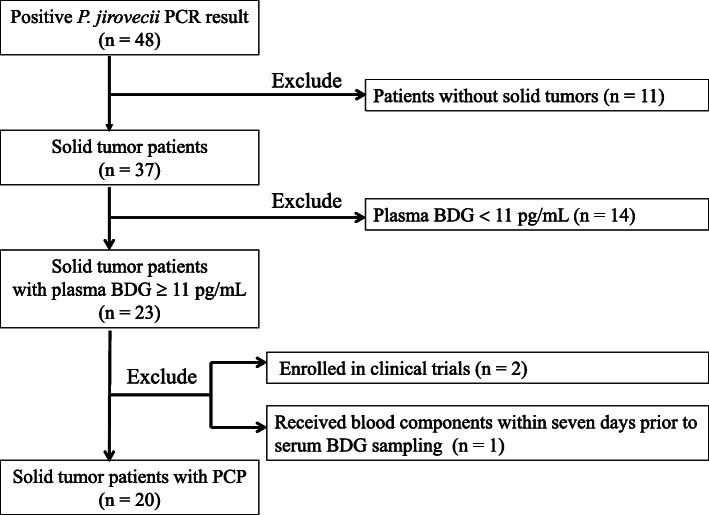
Results: Twenty cases of PCP with solid tumors were documented in 151,718 patients and 788,914 patient-years. Lung cancer (n = 6, 30%) was the most common underlying tumor, followed by breast cancer (n = 3, 15%). Only six (30%) patients were taking a dosage of ≥20 mg prednisone equivalents daily for ≥4 weeks from the onset of PCP. Among the remaining 14 patients, seven (50%) had coexisting pulmonary diseases, 10 (71%) had received chemotherapy within 90 days prior to PCP diagnosis, seven (50%) had undergone chest radiation therapy before PCP diagnosis, seven (50%) had received only intermittent corticosteroids, and one (7%) received no corticosteroids. Mortality attributable to PCP was 40%.
Conclusions: More than half of the patients were not taking a dosage of ≥20 mg prednisone equivalents daily for ≥4 weeks. Multiple other factors (e.g., lymphocytopenia, radiation to chest) may have potentially contributed to PCP in patients with solid tumors in a composite manner. We need to establish a method for estimating the likelihood of PCP taking multiple factors into account in this patient population.
Keywords: Beta-D-glucans; Corticosteroids; Invasive fungal infections; Mycoses; Pneumocystis jirovecii; Solid tumors.
© 2021. The Author(s).
Conflict of interest statement
SH has received honoraria from MSD, Shionogi, Astellas, BD, Beckman Coulter Diagnostics, Sumitomo Dainippon Pharma, and Meiji; has served in a consultancy
Figures
References
-
- Fillatre P, Decaux O, Jouneau S, Revest M, Gacouin A, Robert-Gangneux F, Fresnel A, Guiguen C, le Tulzo Y, Jégo P, Tattevin P. Incidence of pneumocystis jiroveci pneumonia among groups at risk in HIV-negative patients. Am J Med. 2014;127(1242):e11–e17. doi: 10.1016/j.amjmed.2014.07.010. - DOI - PubMed
-
- Roblot F, Le Moal G, Kauffmann-Lacroix C, Bastides F, Boutoille D, Verdon R, et al. Pneumocystis jirovecii pneumonia in HIV-negative patients: a prospective study with focus on immunosuppressive drugs and markers of immune impairment. Scand J Infect Dis. 2014;46(3):210–214. doi: 10.3109/00365548.2013.865142. - DOI - PubMed
-
- Taplitz RA, Kennedy EB, Bow EJ, Crews J, Gleason C, Hawley DK, Langston AA, Nastoupil LJ, Rajotte M, Rolston KV, Strasfeld L, Flowers CR. Antimicrobial prophylaxis for adult patients with cancer-related immunosuppression: ASCO and IDSA clinical practice guideline update. J Clin Oncol. 2018;36(30):3043–3054. doi: 10.1200/JCO.18.00374. - DOI - PubMed
-
- NCCN Clinical Practice Guidelines in Oncology Prevention and Treatment of Cancer-Related Infections. National Comprehensive Cancer Network. Version 1. 2020 https://www.nccn.org/professionals/physician_gls/pdf/infections.pdf. Accessed on Oct 18, 2020.
-
- Classen AY, Henze L, von Lilienfeld-Toal M, Maschmeyer G, Sandherr M, Graeff LD, Alakel N, Christopeit M, Krause SW, Mayer K, Neumann S, Cornely OA, Penack O, Weißinger F, Wolf HH, Vehreschild JJ. Primary prophylaxis of bacterial infections and pneumocystis jirovecii pneumonia in patients with hematologic malignancies and solid tumors: 2020 updated guidelines of the infectious diseases working Party of the German Society of hematology and medical oncology (AGIHO/DGHO) Ann Hematol. 2021;100(6):1603–1620. doi: 10.1007/s00277-021-04452-9. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
