

Prevalence of abnormal cardiovascular magnetic resonance findings in recovered patients from COVID-19: a systematic review and meta-analysis
- PMID: 34479603
- PMCID: PMC8414035
- DOI: 10.1186/s12968-021-00792-7
Prevalence of abnormal cardiovascular magnetic resonance findings in recovered patients from COVID-19: a systematic review and meta-analysis
Abstract
Background: The prevalence of abnormal cardiovascular magnetic resonance (CMR) findings in recovered coronavirus disease 2019 (COVID-19) patients is unclear. This study aimed to investigate the prevalence of abnormal CMR findings in recovered COVID-19 patients.
Methods: A systematic literature search was performed to identify studies that report the prevalence of abnormal CMR findings in recovered COVID-19 patients. The number of patients with abnormal CMR findings and diagnosis of myocarditis on CMR (based on the Lake Louise criteria) and each abnormal CMR parameter were extracted. Subgroup analyses were performed according to patient characteristics (athletes vs. non-athletes and normal vs. undetermined cardiac enzyme levels). The pooled prevalence and 95% confidence interval (CI) of each CMR finding were calculated. Study heterogeneity was assessed, and meta-regression analysis was performed to investigate factors associated with heterogeneity.
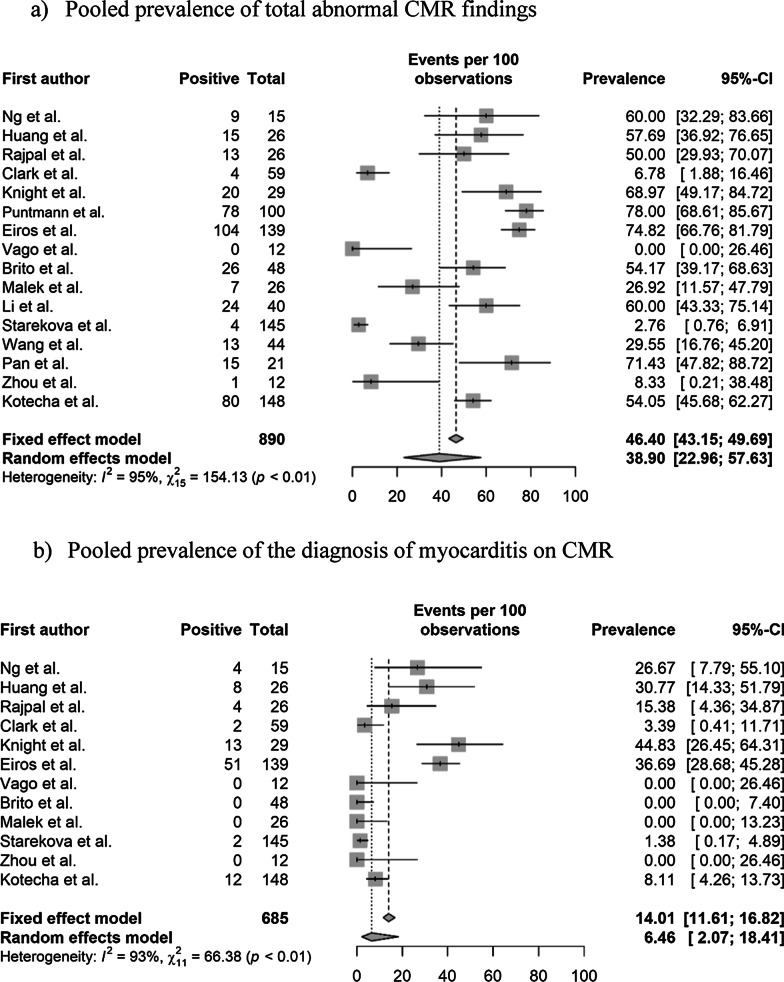
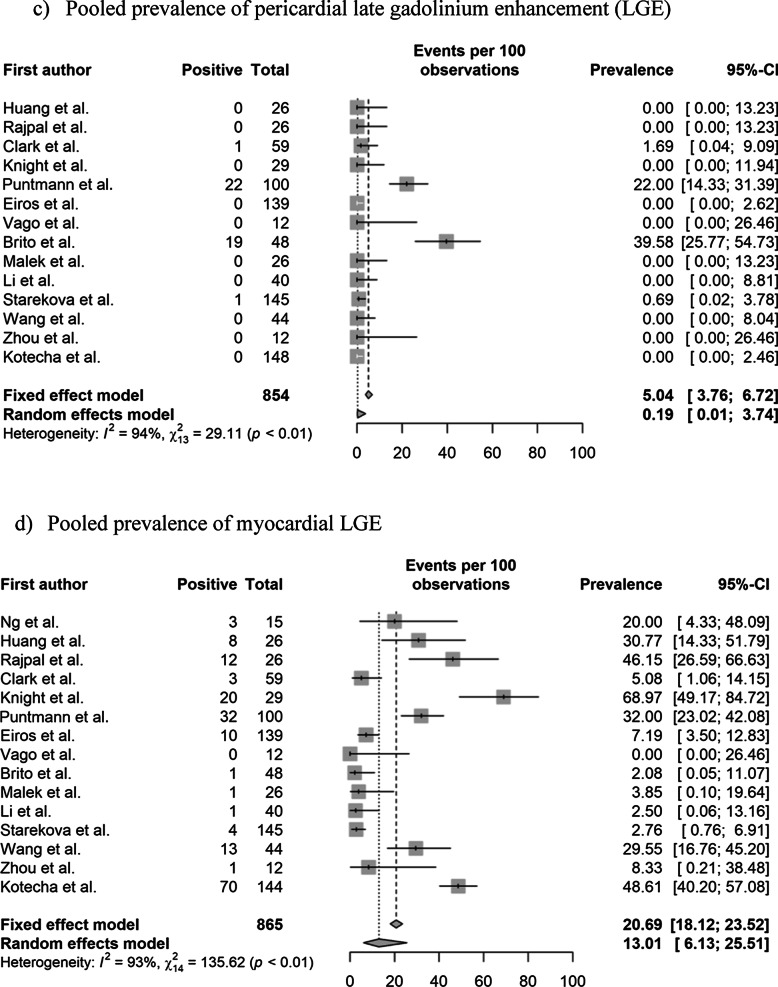
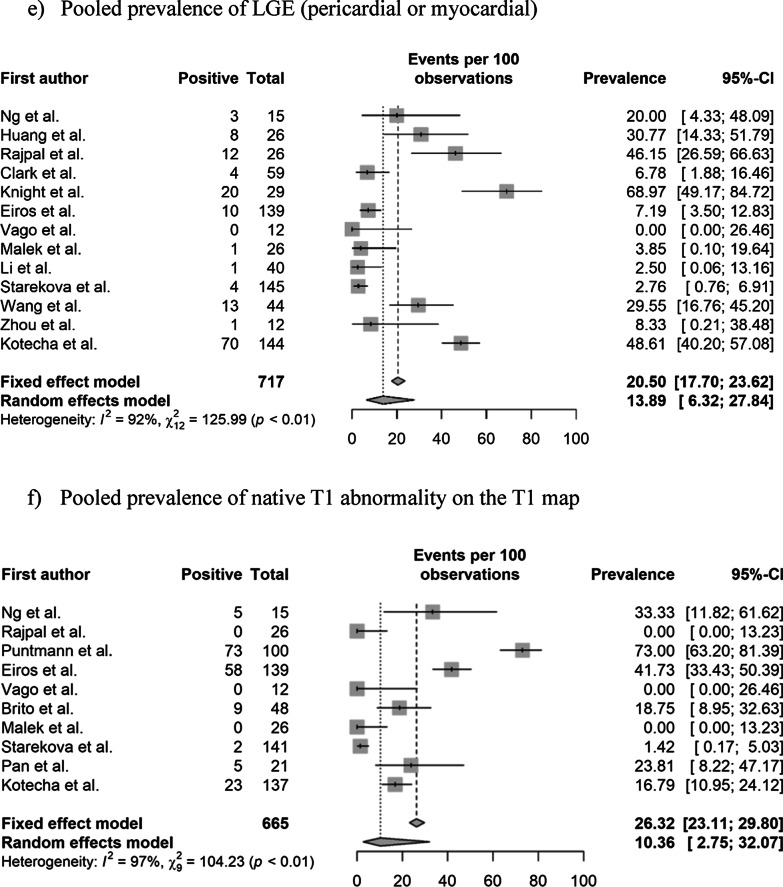
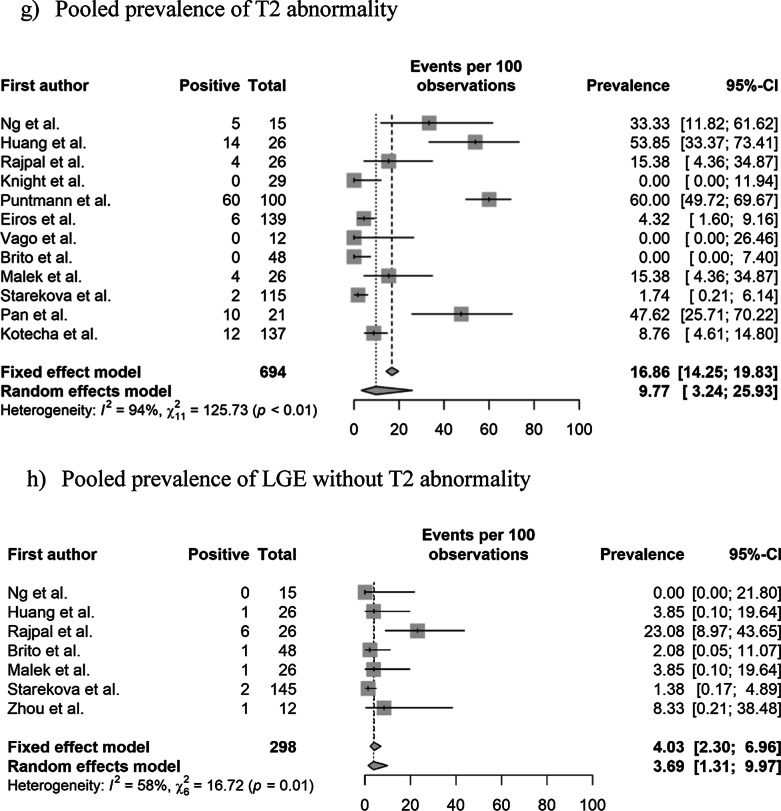
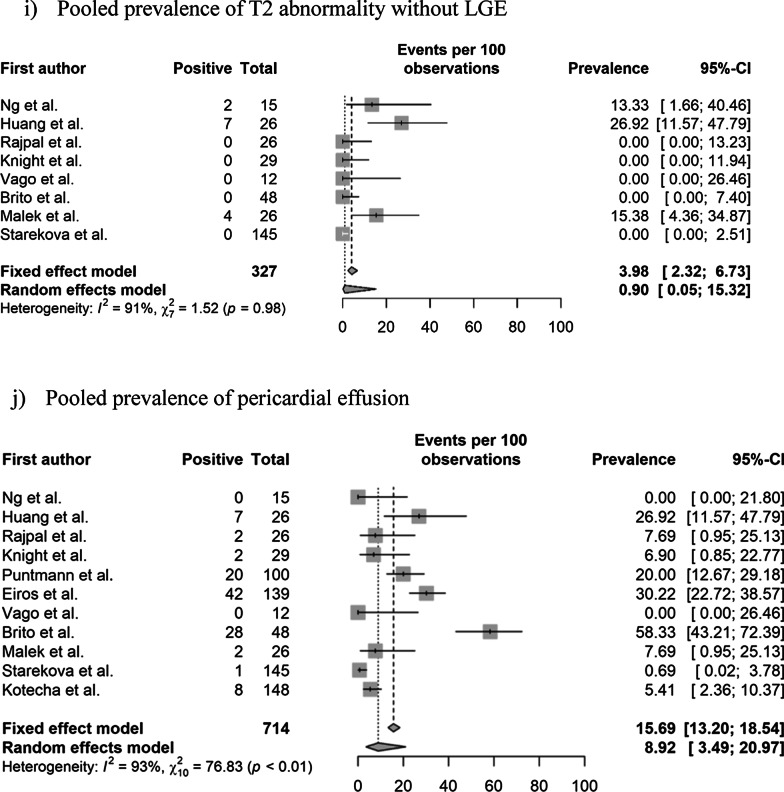
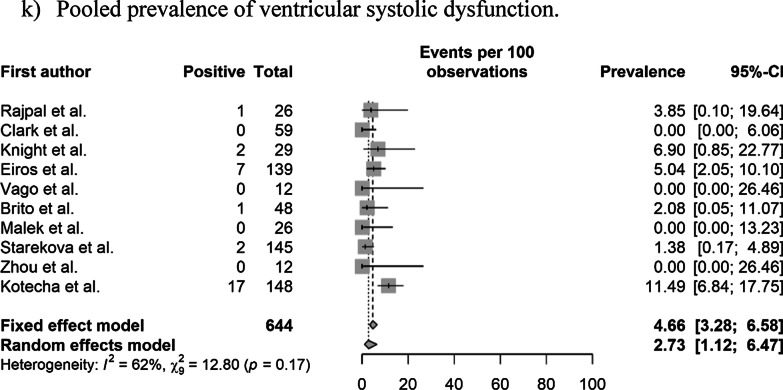
Results: In total, 890 patients from 16 studies were included in the analysis. The pooled prevalence of one or more abnormal CMR findings in recovered COVID-19 patients was 46.4% (95% CI 43.2%-49.7%). The pooled prevalence of myocarditis and late gadolinium enhancement (LGE) was 14.0% (95% CI 11.6%-16.8%) and 20.5% (95% CI 17.7%-23.6%), respectively. Further, heterogeneity was observed (I2 > 50%, p < 0.1). In the subgroup analysis, the pooled prevalence of abnormal CMR findings and myocarditis was higher in non-athletes than in athletes (62.5% vs. 17.1% and 23.9% vs. 2.5%, respectively). Similarly, the pooled prevalence of abnormal CMR findings and LGE was higher in the undetermined than in the normal cardiac enzyme level subgroup (59.4% vs. 35.9% and 45.5% vs. 8.3%, respectively). Being an athlete was a significant independent factor related to heterogeneity in multivariate meta-regression analysis (p < 0.05).
Conclusions: Nearly half of recovered COVID-19 patients exhibited one or more abnormal CMR findings. Athletes and patients with normal cardiac enzyme levels showed a lower prevalence of abnormal CMR findings than non-athletes and patients with undetermined cardiac enzyme levels. Trial registration The study protocol was registered in the PROSPERO database (registration number: CRD42020225234).
Keywords: Cardiac magnetic resonance imaging; Coronavirus disease 2019; Magnetic resonance imaging.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Organization WH. WHO Director-General's opening remarks at the media briefing on COVID-19 - 11 March 2020. 2020.
-
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. Accessed 7 Jul 2021.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
