

Development of preclinical and clinical models for immune-related adverse events following checkpoint immunotherapy: a perspective from SITC and AACR
- PMID: 34479924
- PMCID: PMC8420733
- DOI: 10.1136/jitc-2021-002627
Development of preclinical and clinical models for immune-related adverse events following checkpoint immunotherapy: a perspective from SITC and AACR
Abstract
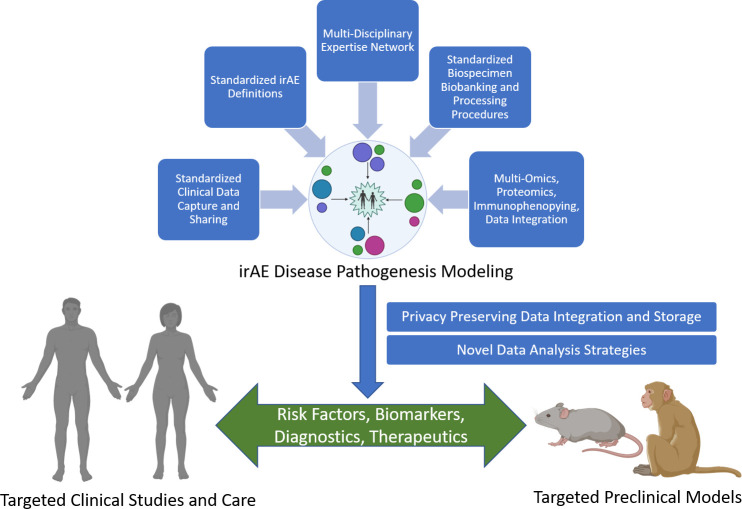
Recent advances in cancer immunotherapy have completely revolutionized cancer treatment strategies. Nonetheless, the increasing incidence of immune-related adverse events (irAEs) is now limiting the overall benefits of these treatments. irAEs are well-recognized side effects of some of the most effective cancer immunotherapy agents, including antibody blockade of the cytotoxic T-lymphocyte-associated protein 4 and programmed death protein 1/programmed-death ligand 1 pathways. To develop an action plan on the key elements needed to unravel and understand the key mechanisms driving irAEs, the Society for Immunotherapy for Cancer and the American Association for Cancer Research partnered to bring together research and clinical experts in cancer immunotherapy, autoimmunity, immune regulation, genetics and informatics who are investigating irAEs using animal models, clinical data and patient specimens to discuss current strategies and identify the critical next steps needed to create breakthroughs in our understanding of these toxicities. The genetic and environmental risk factors, immune cell subsets and other key immunological mediators and the unique clinical presentations of irAEs across the different organ systems were the foundation for identifying key opportunities and future directions described in this report. These include the pressing need for significantly improved preclinical model systems, broader collection of biospecimens with standardized collection and clinical annotation made available for research and integration of electronic health record and multiomic data with harmonized and standardized methods, definitions and terminologies to further our understanding of irAE pathogenesis. Based on these needs, this report makes a set of recommendations to advance our understanding of irAE mechanisms, which will be crucial to prevent their occurrence and improve their treatment.
Keywords: autoimmunity; immunotherapy; translational medical research.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: JAB is a cofounder, CEO and a Board member of Sonoma Biotherapeutics (with salary and ownership interests). He is a cofounder of Celsius Therapeutics with ownership interests; a member of the Board of Directors of Gilead and Provention Bio with compensation and ownership interests, and the Parker Institute for Cancer Immunotherapy; and is a member of the scientific advisory boards of Arcus Biosciences, Solid Biosciences, Rheos Medicines and Vir Biotechnology. LHB has received consulting fees from Calidi, Takeda, Western Oncolytics, Khloris, Pyxis, Cytomix, Roche-Genentech, DC Prime and RAPT in the last 24 months. EMJ is a paid consultant for Adaptive Biotech, CSTONE, Achilles, DragonFly, Candel Therapeutics and Genocea. She receives funding from Lustgarten Foundation and Bristol Myer Squibb. She is the Chief Medical Advisor for Lustgarten and SAB advisor to the Parker Institute for Cancer Immunotherapy (PICI) and for the C3 Cancer Institute. She is a founding member of Abmeta. AHS receives royalty from Pfizer; has IP rights with Roche, Merck, Bristol Myers Squibb, EMD-Serono, Boehringer-Ingelheim, AstraZeneca, Dako and Novartis; receives consulting fees from Surface Oncology, Elstar, SQZ Biotechnologies, Selecta, Elpiscience, Monopteros, Bicara, GlaxoSmithKline and Janssen advisory boards, the Stand Up to Cancer Grant Catalyst Executive Advisory Committee and Review Panel, the Bloomberg Kimmel Institute for Cancer Immunotherapy at Johns Hopkins EAB, the Human Oncology and Pathogenesis Program at Memorial Sloan Kettering Cancer Center EAB, and the Massachusetts General Hospital Cancer Center EAB; has contracted research with Roche, Merck, AbbVie and Quark Ventures; has partner consulting fees from Roche, Bristol Myers Squibb, Xios and Origimed; and has partner ownership interest in Nextpoint, Triursus and Xios. All other authors have nothing to disclose. SITC staff (EBS) has nothing to disclose.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials