

Genetic profiles of Barrett's esophagus and esophageal adenocarcinoma in Japanese patients
- PMID: 34480065
- PMCID: PMC8417273
- DOI: 10.1038/s41598-021-97249-9
Genetic profiles of Barrett's esophagus and esophageal adenocarcinoma in Japanese patients
Abstract
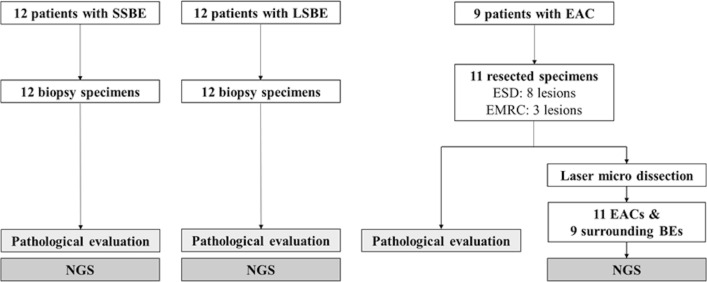
The genetic characteristics of Barrett's esophagus (BE) and esophageal adenocarcinoma (EAC) in the Japanese population is unclear. This study aims to investigate the genetic characteristics from nondysplastic BE (NDBE) to early EAC in Japan. Clinical information was collected. Moreover, the genetic profile of NDBE without concurrent dysplasia, early EAC, and surrounding BE were also investigated using endoscopic biopsy samples and formalin-fixed, paraffin-embedded specimens from Japanese patients by targeted next-generation sequencing. Immunohistochemical staining for p53 was also performed for EAC lesions. Targeted NGS was performed for 33 cases with 77 specimens. No significant difference exists in the NDBE group between the number of putative drivers per lesion in the short-segment Barrett's esophagus (SSBE) and long-segment Barrett's esophagus (LSBE) [0 (range, 0-1) vs. 0 (range, 0-1). p = 1.00]. TP53 putative drivers were found in two patients (16.7%) with nondysplastic SSBE. TP53 was the majority of putative drivers in both BE adjacent to EAC and EAC, accounting for 66.7% and 66.7%, respectively. More putative drivers per lesion were found in the EAC than in the NDBE group [1 (range, 0-3) vs. 0 (range, 0-1). p < 0.01]. The genetic variants of TP53 in the Japanese early EAC were similar to those in western countries. However, TP53 putative drivers were detected even in Japanese patients with nondysplastic SSBE. This is significant because such nondysplastic SSBE might have higher risk of progressing to high-grade dysplasia or EAC. The risks of progression may not be underestimated and appropriate follow-ups may be necessary even in patients with SSBE.Trial registration: This study was registered at the University Hospital Medical Information Network (UMIN000034247).
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures




References
-
- Barrett NR. The lower esophagus lined by columnar epithelium. Surgery. 1957;41:881–894. - PubMed
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
