

Efficacy and safety of baricitinib for the treatment of hospitalised adults with COVID-19 (COV-BARRIER): a randomised, double-blind, parallel-group, placebo-controlled phase 3 trial
- PMID: 34480861
- PMCID: PMC8409066
- DOI: 10.1016/S2213-2600(21)00331-3
Efficacy and safety of baricitinib for the treatment of hospitalised adults with COVID-19 (COV-BARRIER): a randomised, double-blind, parallel-group, placebo-controlled phase 3 trial
Erratum in
-
Correction to Lancet Respir Med 2021; published online Sept 1. https://doi.org/10.1016/S2213-2600(21)00331-3.Lancet Respir Med. 2021 Oct;9(10):e102. doi: 10.1016/S2213-2600(21)00410-0. Epub 2021 Sep 8. Lancet Respir Med. 2021. PMID: 34508656 Free PMC article. No abstract available.
Abstract
Background: Baricitinib is an oral selective Janus kinase 1/2 inhibitor with known anti-inflammatory properties. This study evaluates the efficacy and safety of baricitinib in combination with standard of care for the treatment of hospitalised adults with COVID-19.
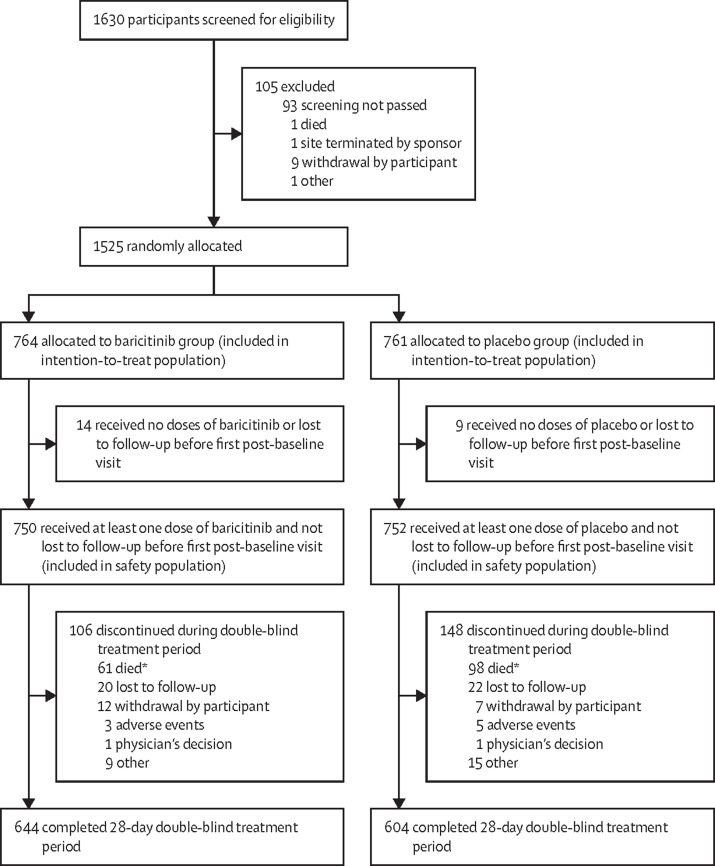
Methods: In this phase 3, double-blind, randomised, placebo-controlled trial, participants were enrolled from 101 centres across 12 countries in Asia, Europe, North America, and South America. Hospitalised adults with COVID-19 receiving standard of care were randomly assigned (1:1) to receive once-daily baricitinib (4 mg) or matched placebo for up to 14 days. Standard of care included systemic corticosteroids, such as dexamethasone, and antivirals, including remdesivir. The composite primary endpoint was the proportion who progressed to high-flow oxygen, non-invasive ventilation, invasive mechanical ventilation, or death by day 28, assessed in the intention-to-treat population. All-cause mortality by day 28 was a key secondary endpoint, and all-cause mortality by day 60 was an exploratory endpoint; both were assessed in the intention-to-treat population. Safety analyses were done in the safety population defined as all randomly allocated participants who received at least one dose of study drug and who were not lost to follow-up before the first post-baseline visit. This study is registered with ClinicalTrials.gov, NCT04421027.
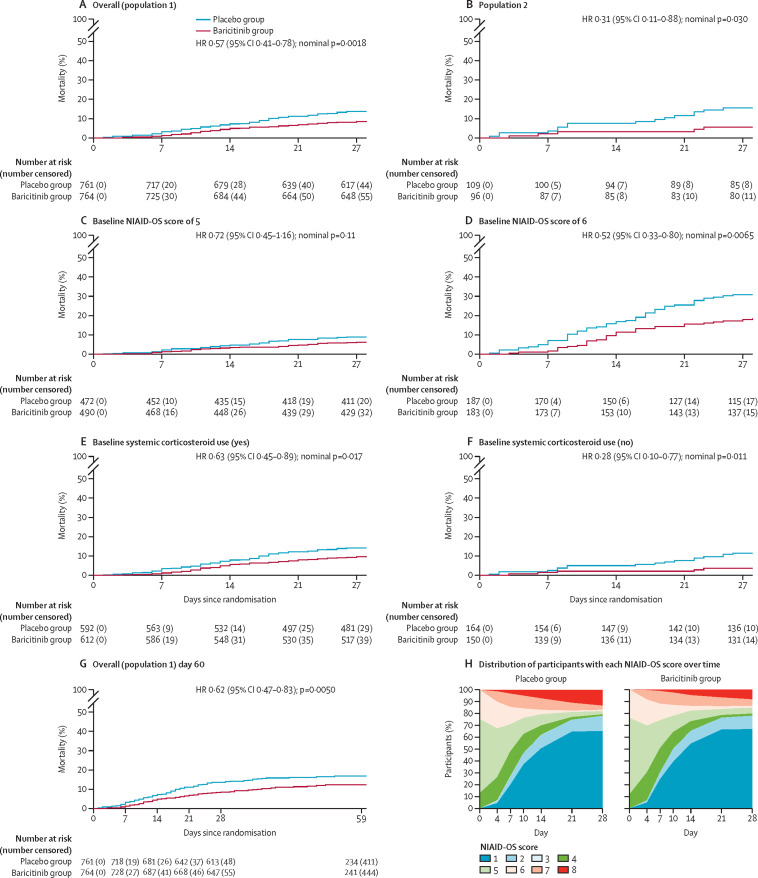
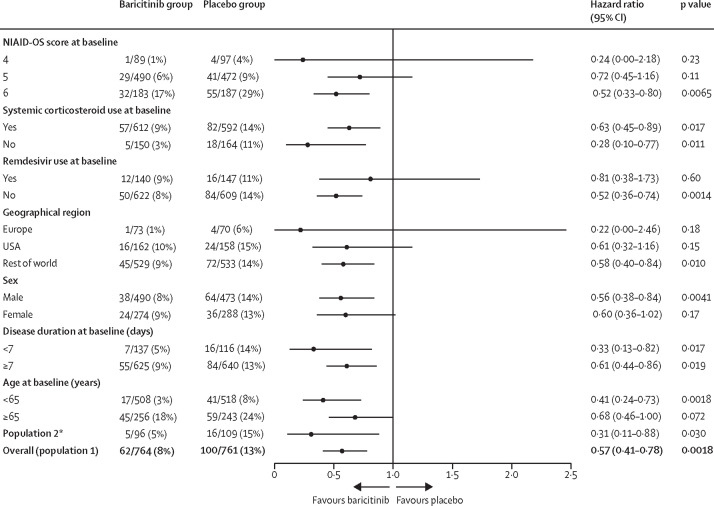
Findings: Between June 11, 2020, and Jan 15, 2021, 1525 participants were randomly assigned to the baricitinib group (n=764) or the placebo group (n=761). 1204 (79·3%) of 1518 participants with available data were receiving systemic corticosteroids at baseline, of whom 1099 (91·3%) were on dexamethasone; 287 (18·9%) participants were receiving remdesivir. Overall, 27·8% of participants receiving baricitinib and 30·5% receiving placebo progressed to meet the primary endpoint (odds ratio 0·85 [95% CI 0·67 to 1·08], p=0·18), with an absolute risk difference of -2·7 percentage points (95% CI -7·3 to 1·9). The 28-day all-cause mortality was 8% (n=62) for baricitinib and 13% (n=100) for placebo (hazard ratio [HR] 0·57 [95% CI 0·41-0·78]; nominal p=0·0018), a 38·2% relative reduction in mortality; one additional death was prevented per 20 baricitinib-treated participants. The 60-day all-cause mortality was 10% (n=79) for baricitinib and 15% (n=116) for placebo (HR 0·62 [95% CI 0·47-0·83]; p=0·0050). The frequencies of serious adverse events (110 [15%] of 750 in the baricitinib group vs 135 [18%] of 752 in the placebo group), serious infections (64 [9%] vs 74 [10%]), and venous thromboembolic events (20 [3%] vs 19 [3%]) were similar between the two groups.
Interpretation: Although there was no significant reduction in the frequency of disease progression overall, treatment with baricitinib in addition to standard of care (including dexamethasone) had a similar safety profile to that of standard of care alone, and was associated with reduced mortality in hospitalised adults with COVID-19.
Funding: Eli Lilly and Company.
Translations: For the French, Japanese, Portuguese, Russian and Spanish translations of the abstract see Supplementary Materials section.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests VCM received research grants from the US Centers for Disease Control and Prevention (CDC), Gilead Sciences, the US National Institutes of Health (NIH), Veterans Affairs, and ViiV; received honoraria from Eli Lilly and Company; served as an advisory board member for Eli Lilly and Company and Novartis; and participated as a study section chair for the NIH. AVR received research grants from Eli Lilly and Company; and served as a speaker or consultant for AbbVie, Eli Lilly and Company, Novartis, Pfizer, Roche, Sobi, and Union Chimique Belge. SB, CEK, VK, RL, MLBP, AC, SC, BC, PR, XZ, and DHA are employees and shareholders of Eli Lilly and Company. JDG received research support from Eli Lilly and Company, Regeneron Pharmaceuticals, and Gilead Sciences; grants from Eurofins Viracor and the Biomedical Advanced Research and Development Authority (administered by Merck); speaker fees from Eli Lilly and Company, Gilead Sciences, and Mylan Pharmaceuticals; and advisory board fees from Gilead Sciences. JAA served as a speaker and scientific advisor for AstraZeneca, Boehringer Ingelheim, BMS, Eli Lilly and Company, Foundation Medicine, Novartis, MSD, Roche, and Takeda. VE received a research grant from Eli Lilly and Company. MS received research grants from Eli Lilly and Company, NIAID, and Novartis; and served as a board member for NBOME, Osteopathic Founders Foundation, and COGMED. EWE received research grants from the CDC, NIH, and Veterans Affairs; and served as an unpaid consultant for Eli Lilly and Company. RDP declares no competing interests
Figures
Comment in
-
Baricitinib: the first immunomodulatory treatment to reduce COVID-19 mortality in a placebo-controlled trial.Lancet Respir Med. 2021 Dec;9(12):1349-1351. doi: 10.1016/S2213-2600(21)00358-1. Epub 2021 Sep 1. Lancet Respir Med. 2021. PMID: 34480862 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
