

Molecular Characterization of Limited Ulcerative Colitis Reveals Novel Biology and Predictors of Disease Extension
- PMID: 34480882
- PMCID: PMC8640960
- DOI: 10.1053/j.gastro.2021.08.053
Molecular Characterization of Limited Ulcerative Colitis Reveals Novel Biology and Predictors of Disease Extension
Abstract
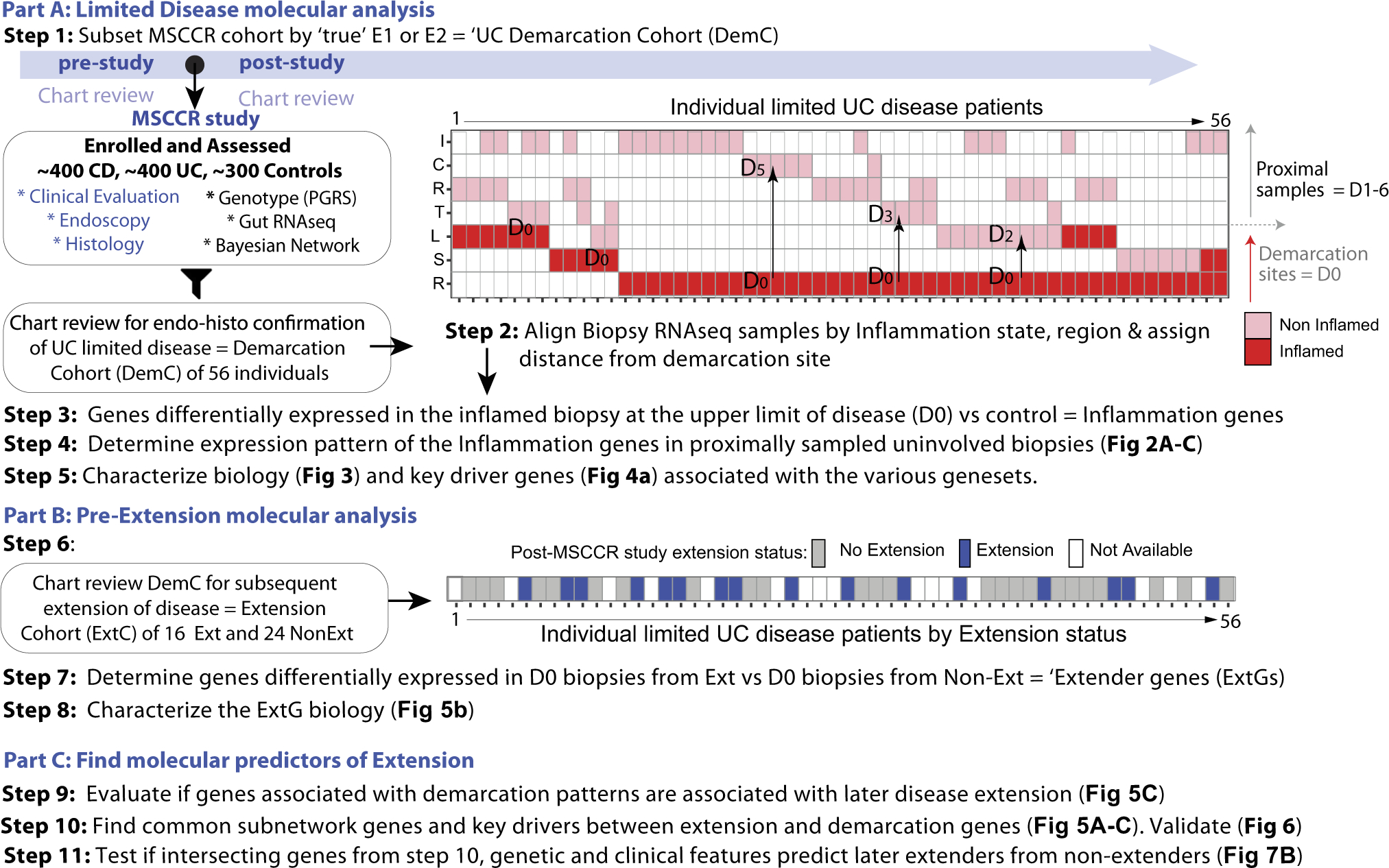
Background and aims: Disease extent varies in ulcerative colitis (UC) from proctitis to left-sided colitis to pancolitis and is a major prognostic factor. When the extent of UC is limited there is often a sharp demarcation between macroscopically involved and uninvolved areas and what defines this or subsequent extension is unknown. We characterized the demarcation site molecularly and determined genes associated with subsequent disease extension.
Methods: We performed RNA sequence analysis of biopsy specimens from UC patients with endoscopically and histologically confirmed limited disease, of which a subset later extended. Biopsy specimens were obtained from the endoscopically inflamed upper (proximal) limit of disease, immediately adjacent to the uninvolved colon, as well as at more proximal, endoscopically uninflamed colonic segments.
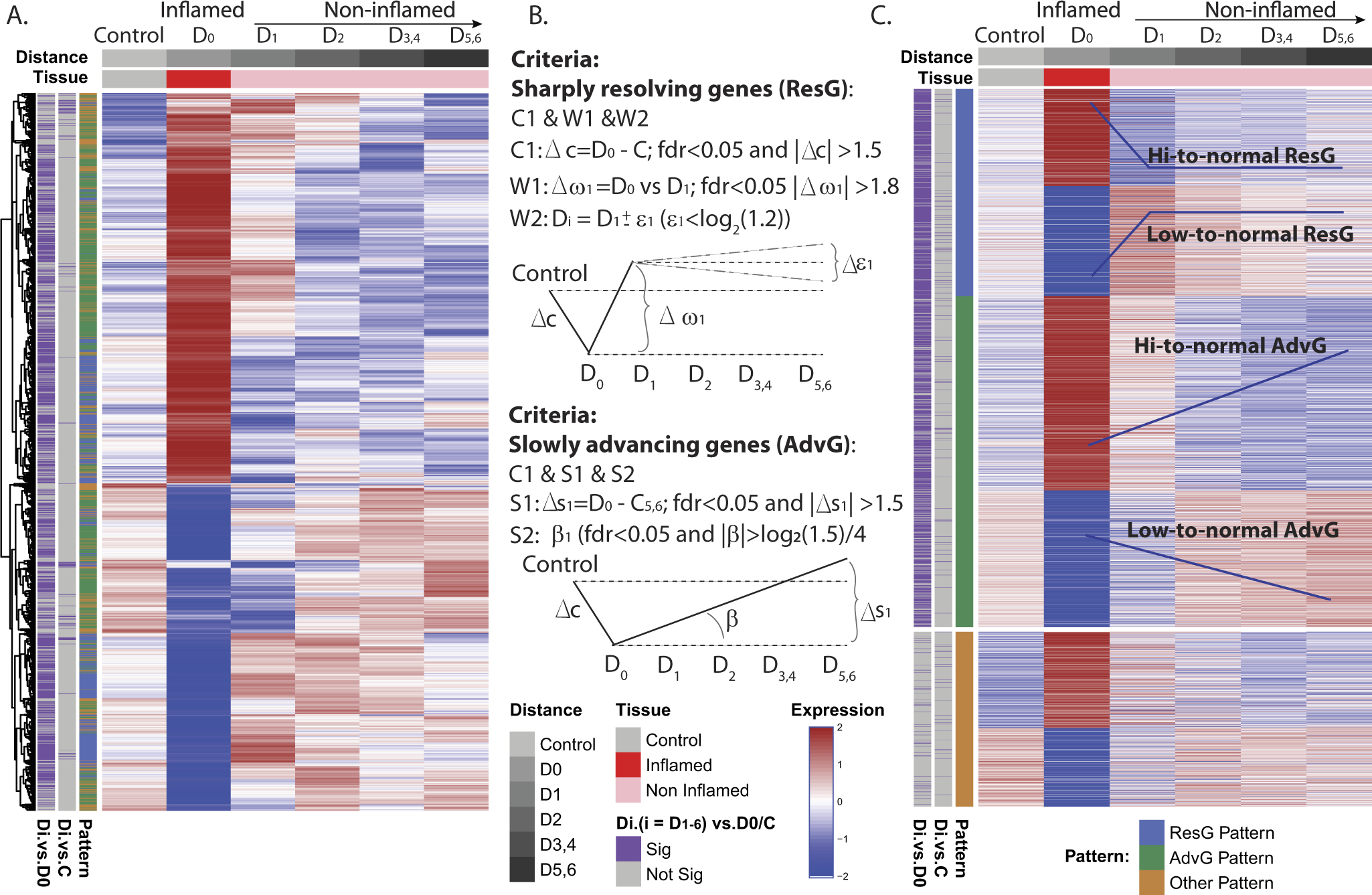
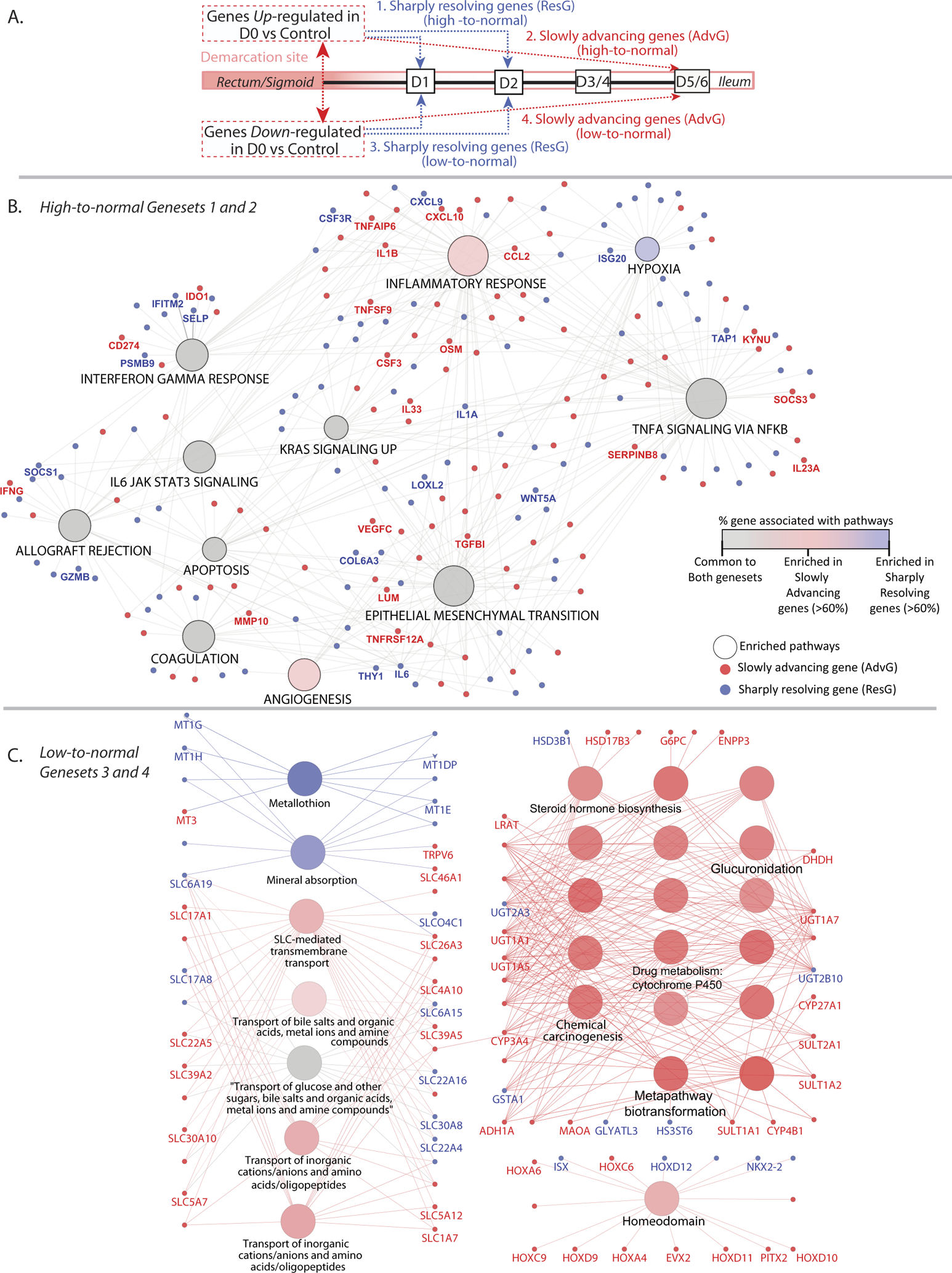
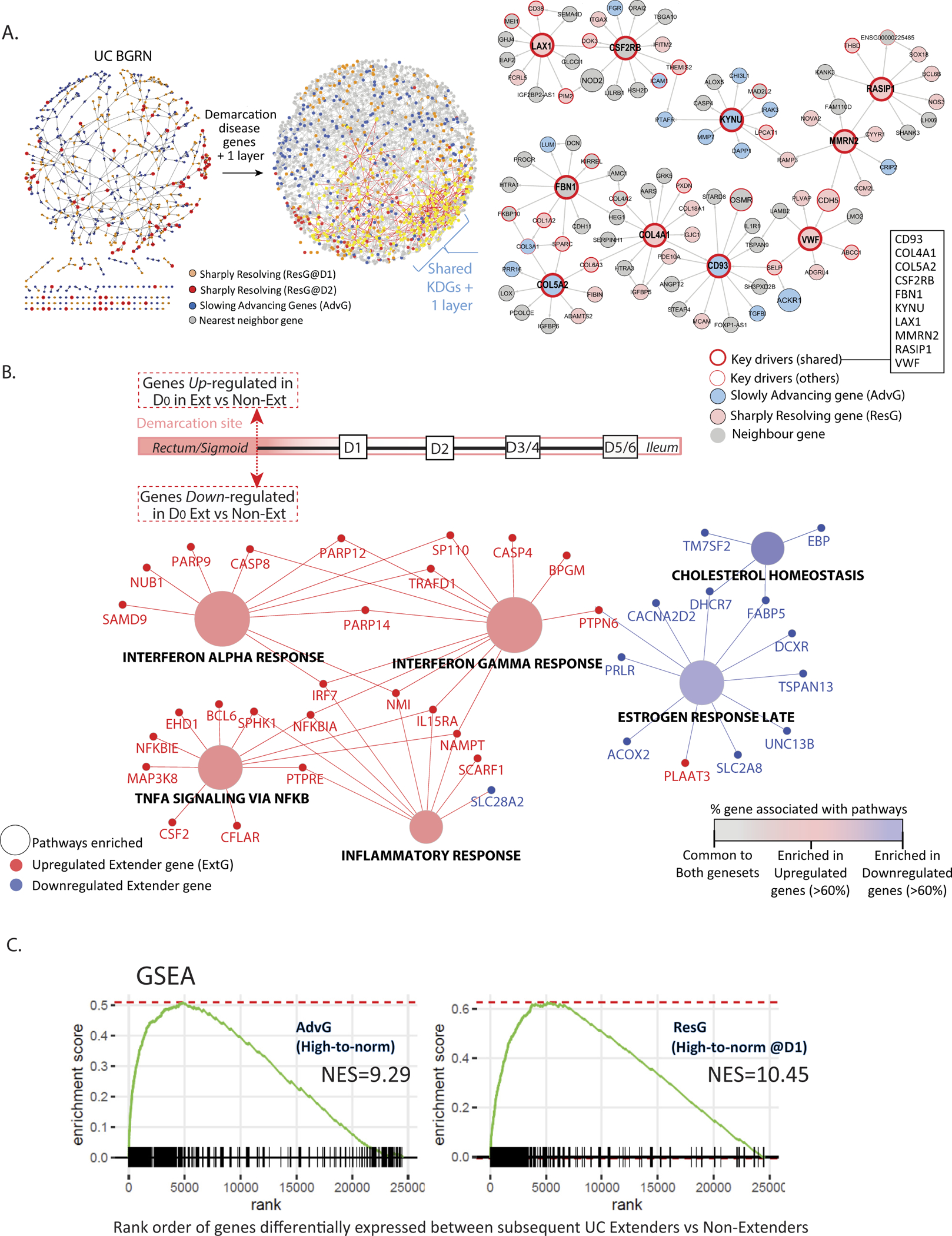
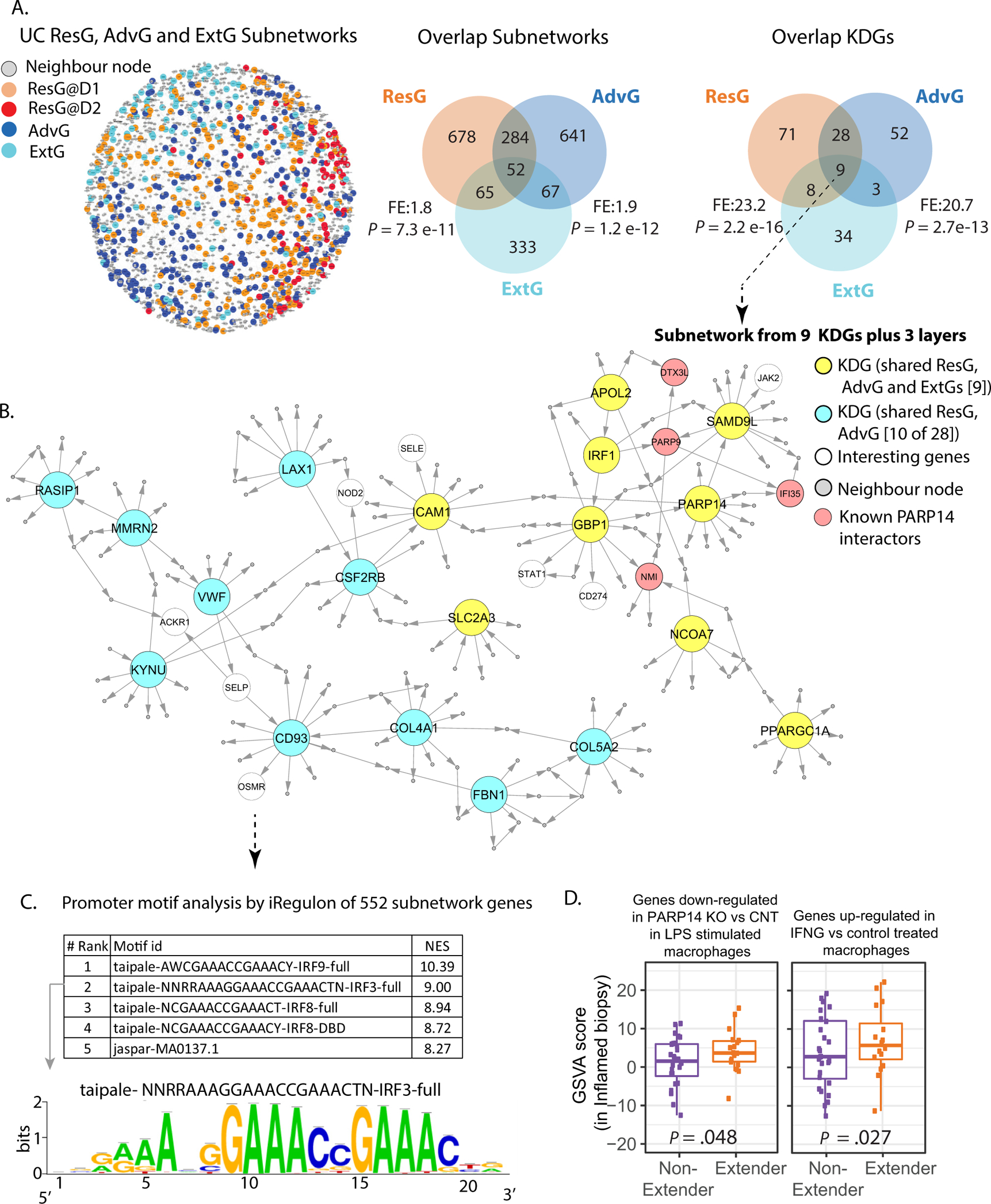
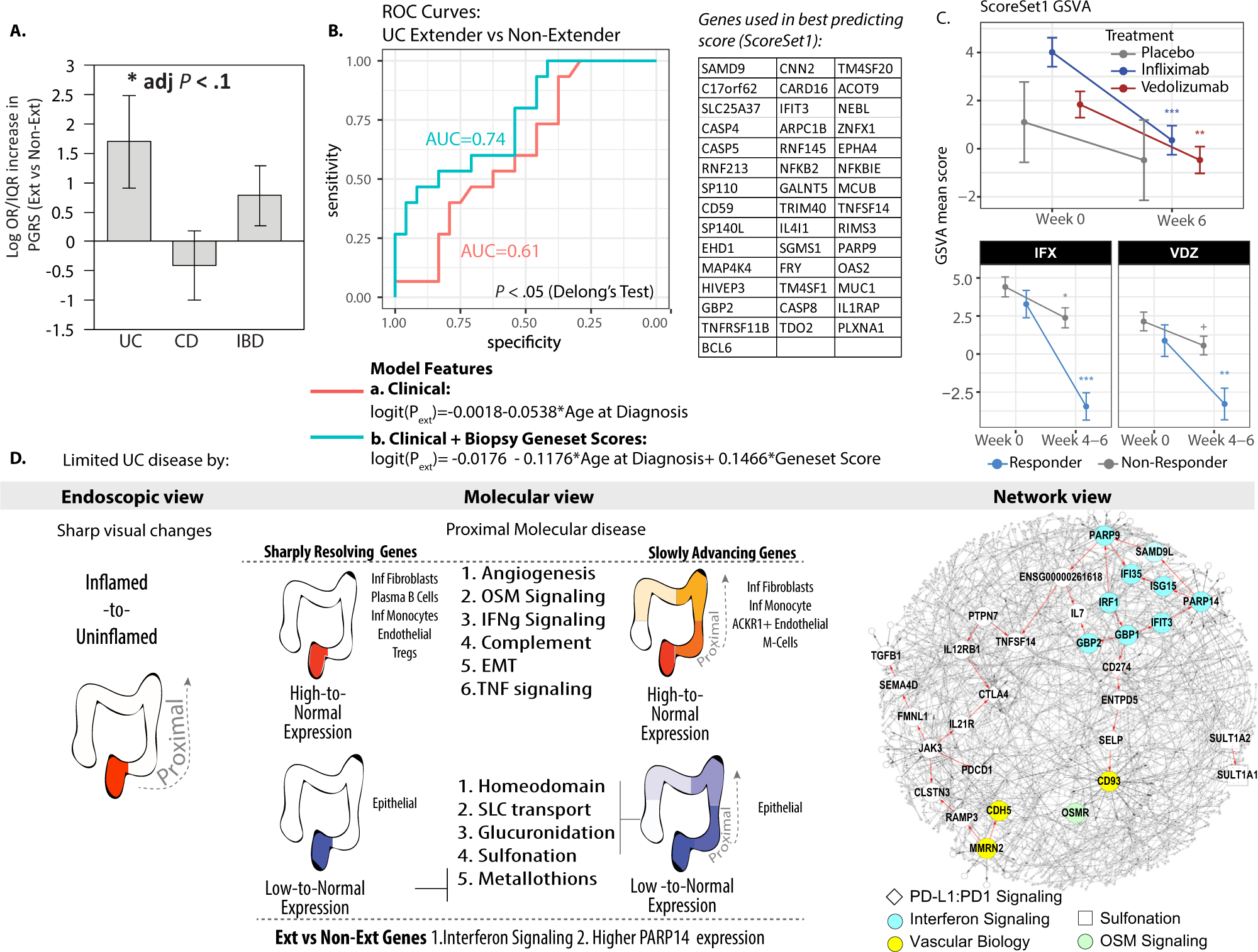
Results: Differentially expressed genes were identified in the endoscopically inflamed biopsy specimens taken at each patient's most proximal diseased site relative to healthy controls. Expression of these genes in the more proximal biopsy specimens transitioned back to control levels abruptly or gradually, the latter pattern supporting the concept that disease exists beyond the endoscopic disease demarcation site. The gradually transitioning genes were associated with inflammation, angiogenesis, glucuronidation, and homeodomain pathways. A subset of these genes in inflamed biopsy specimens was found to predict disease extension better than clinical features and were responsive to biologic therapies. Network analysis revealed critical roles for interferon signaling in UC inflammation and poly(ADP-ribose) polymerase 14 (PARP14) was a predicted key driver gene of extension. Higher PARP14 protein levels were found in inflamed biopsy specimens of patients with limited UC that subsequently extended.
Conclusion: Molecular predictors of disease extension reveal novel strategies for disease prognostication and potential therapeutic targeting.
Keywords: Disease Extension; Interferon Signaling; Molecular; PARP14; UC.
Copyright © 2021 AGA Institute. Published by Elsevier Inc. All rights reserved.
Figures

References
-
- Silverberg MS, Satsangi J, Ahmad T, et al. Toward an integrated clinical, molecular and serological classification of inflammatory bowel disease: report of a Working Party of the 2005 Montreal World Congress of Gastroenterology. Can J Gastroenterol 2005;19(Suppl A):5A–36A. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
