

Vaginal delivery of vaccines
- PMID: 34481031
- PMCID: PMC8722700
- DOI: 10.1016/j.addr.2021.113956
Vaginal delivery of vaccines
Abstract
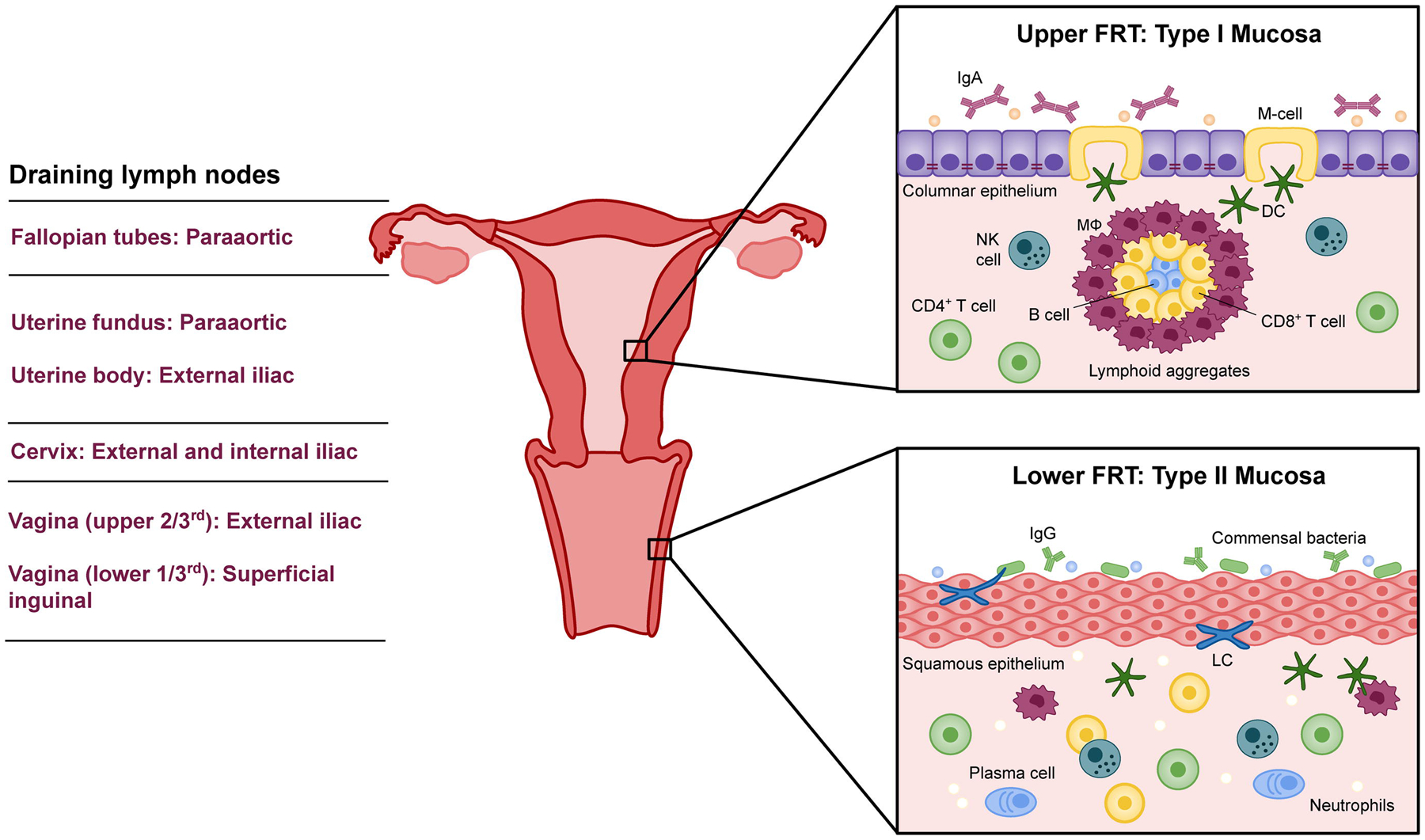
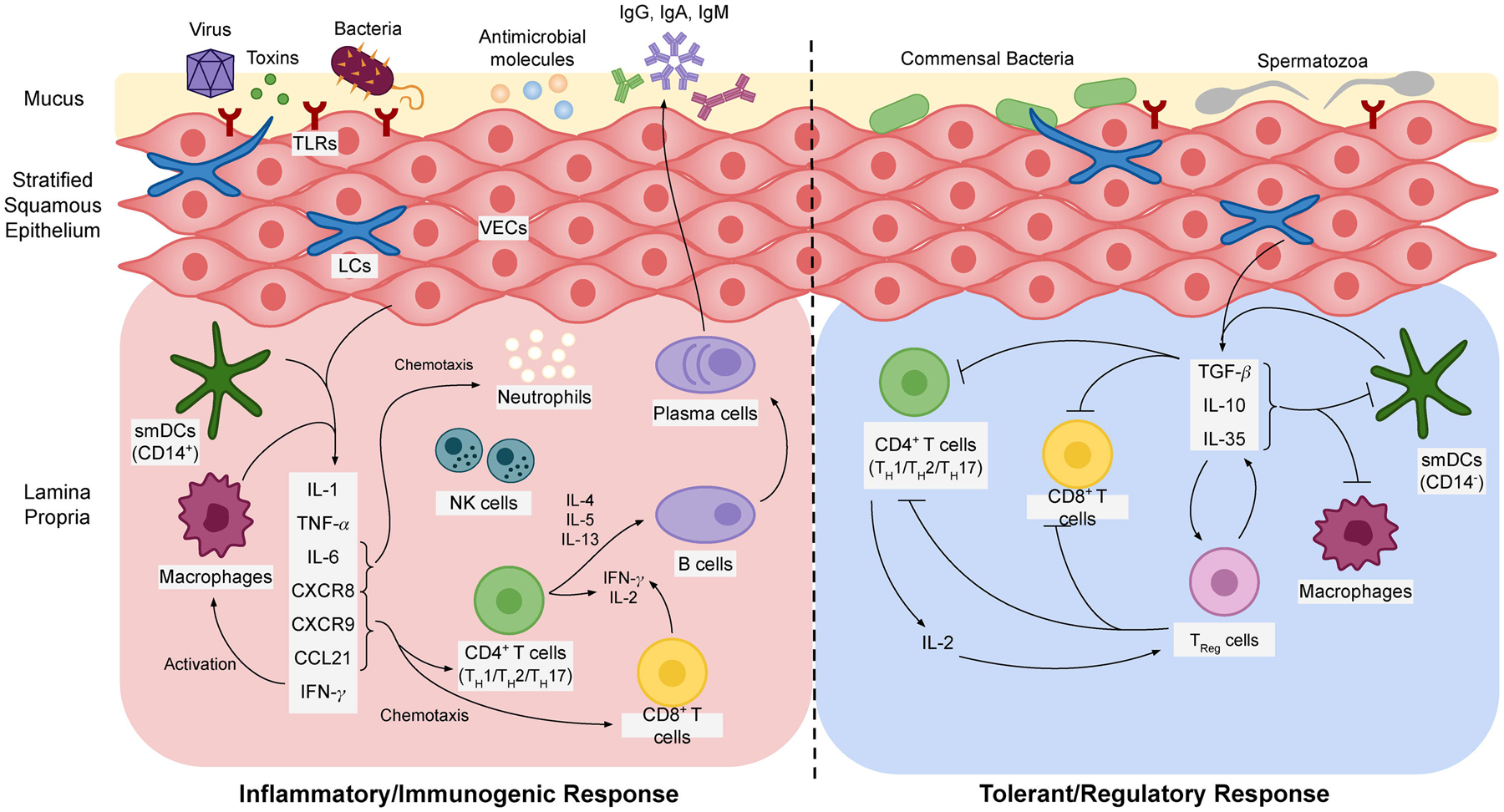
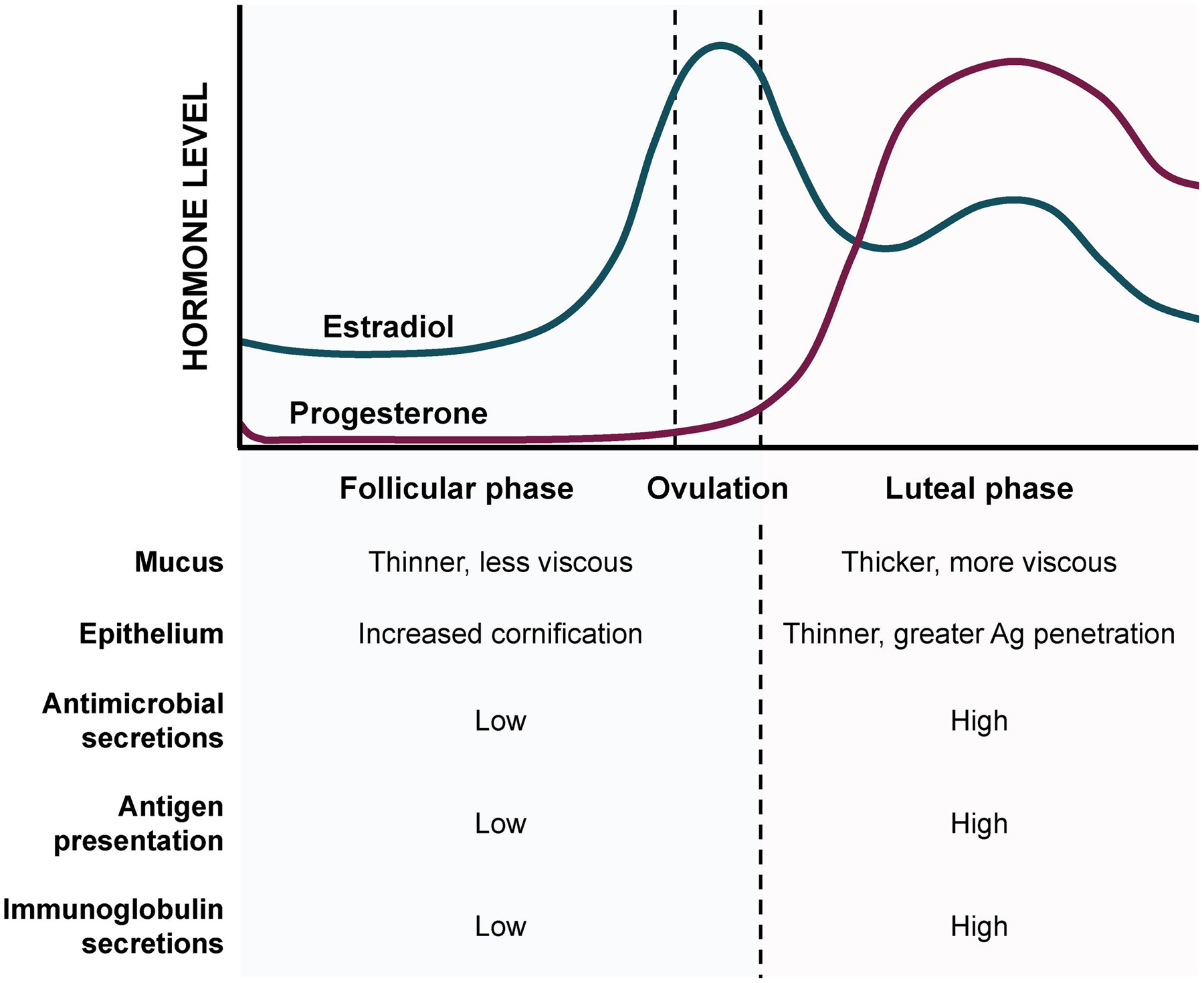
Recent estimates suggest that one in two sexually active individuals will acquire a sexually transmitted infection by age 25, an alarming statistic that amounts to over 1 million new infections per day worldwide. Vaccination against STIs is highly desirable for alleviating this global burden of disease. Vaginal immunization is a promising strategy to combat transmission via the vaginal mucosa. The vagina is typically considered a poor inductive site for common correlates of adaptive immunity. However, emerging evidence suggests that immune tolerance may be overcome by precisely engineered vaccination schemes that orchestrate cell-mediated immunity and establish tissue resident memory immune cells. In this review, we will discuss the unique immunological milieu of the vaginal mucosa and our current understanding of correlates of pathogenesis and protection for several common STIs. We then present a summary of recent vaginal vaccine studies and explore the role that mucosal adjuvants and delivery systems play in enhancing protection according to requisite features of immunity. Finally, we offer perspectives on the challenges and future directions of vaginal vaccine delivery, discussing remaining physiological barriers and innovative vaccine formulations that may overcome them.
Keywords: Drug delivery; Mucosal adjuvants; Mucosal immunology; Sexually transmitted infections; Vaginal vaccines.
Copyright © 2021 Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
