

Secukinumab in non-radiographic axial spondyloarthritis: subgroup analysis based on key baseline characteristics from a randomized phase III study, PREVENT
- PMID: 34481517
- PMCID: PMC8418044
- DOI: 10.1186/s13075-021-02613-9
Secukinumab in non-radiographic axial spondyloarthritis: subgroup analysis based on key baseline characteristics from a randomized phase III study, PREVENT
Abstract
Background: To investigate the efficacy of secukinumab in patients with active non-radiographic axial spondyloarthritis (nr-axSpA) grouped by disease activity as assessed by C-reactive protein (CRP) levels and/or magnetic resonance imaging (MRI) scores, human leukocyte antigen (HLA)-B27 status, and sex.
Methods: The phase III PREVENT study randomized (1:1:1) 555 patients to receive subcutaneous secukinumab 150 mg with (LD) or without (NL) loading dose or placebo weekly, followed by every 4 weeks starting at week 4. Here, we report the results of a post hoc analysis reporting the efficacy outcomes (pooled secukinumab) to 16 weeks by CRP, MRI, HLA-B27, and sex.
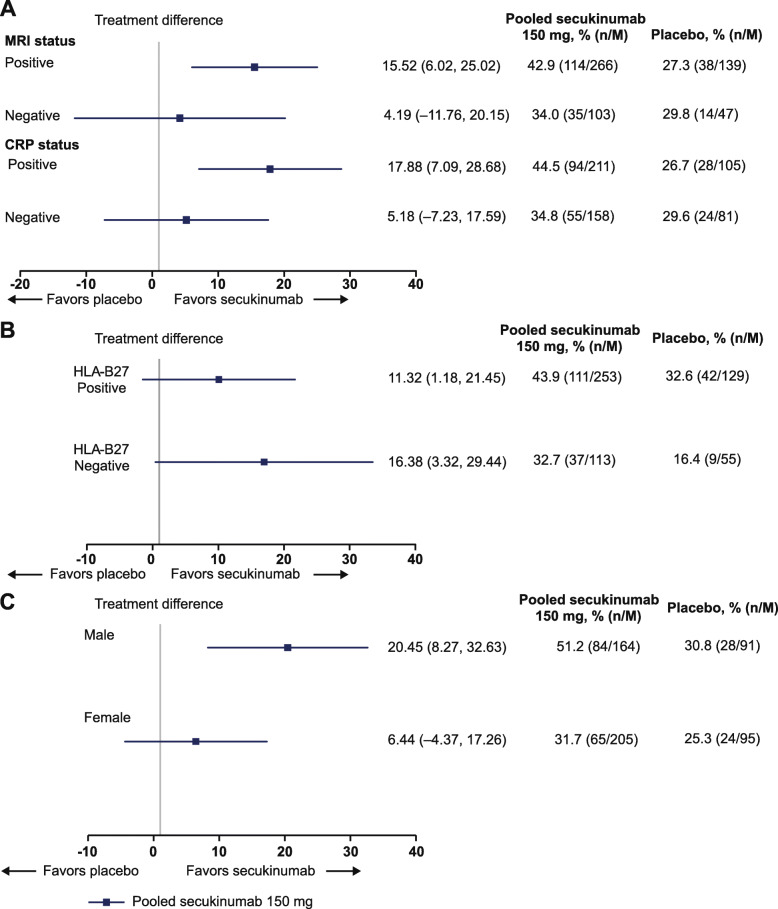
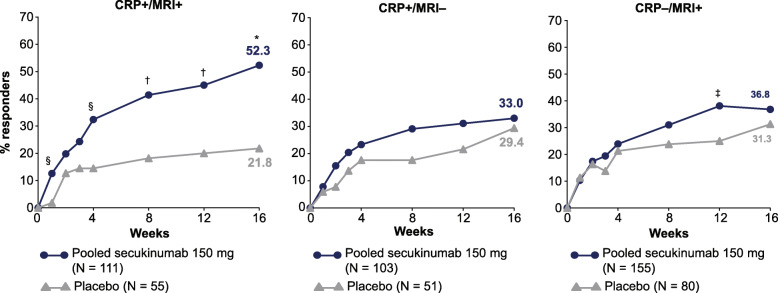
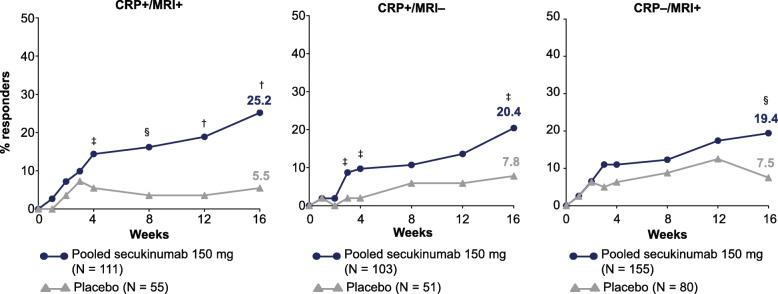
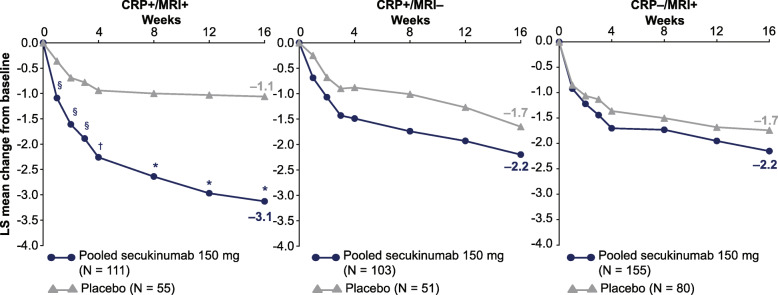
Results: Efficacy differences between the secukinumab and the placebo groups were highest in the CRP+, MRI+, HLA-B27+, and male subgroups, particularly for Ankylosing Spondylitis Disease Activity Score-CRP inactive disease and Assessment of SpondyloArthritis international Society (ASAS) partial remission outcomes. ASAS40 response rates in the CRP+/MRI+ subgroup was 52.3% (secukinumab) versus 21.8% (placebo; P < 0.0001) at week 16. ASAS40 response rates (secukinumab versus placebo) were 43.9% versus 32.6% in HLA-B27+, 32.7% versus 16.4% in HLA-B27- subgroups, 51.2% versus 30.8% in male, and 31.7% versus 25.3% in female patients, respectively.
Conclusions: Secukinumab improved the signs and symptoms of nr-axSpA across patients grouped by CRP (+/-) and/or MRI (+/-) status, HLA-B27 (+/-) status, and sex. The highest treatment differences between secukinumab and placebo were observed in patients with both elevated CRP and evidence of sacroiliitis on MRI. Treatment difference was minimal between HLA-B27 (+) and (-) subgroups. Male patients had higher relative responses than female patients.
Trial registration: ClinicalTrials.gov , NCT02696031 . Registered on 02 March 2016.
Keywords: Biologicals; C-reactive protein; Gender; Human leukocyte antigen B27; Interleukins; Magnetic resonance imaging; Non-radiographic axial spondyloarthritis.
© 2021. The Author(s).
Conflict of interest statement
JB reports grant/research support from AbbVie, Amgen, BMS, Boehringer, Celgene, Celltrion, Centocor, Chugai, Medac, MSD, Mundipharma, Novartis, Pfizer, Roche, Sanofi-Aventis, and UCB; consultation fees from AbbVie, Amgen, BMS, Boehringer, Celgene, Celltrion, Centocor, Chugai, EBEWE Pharma, Medac, MSD, Mundipharma, Novartis, Pfizer, Roche, Sanofi-Aventis, and UCB; and speakers bureau fees from AbbVie, Amgen, BMS, Boehringer, Celgene, Celltrion, Centocor, Chugai, EBEWE Pharma, Medac, MSD, Mundipharma, Novartis, Pfizer, Roche, Sanofi-Aventis, and UCB. RB reports research grants from AbbVie, MSD, and Roche; consulting fees from AbbVie, Pfizer, Roche, Bristol-Myers, Janssen, and MSD; and speakers bureau fees from AbbVie, Pfizer, Roche, Bristol-Myers, Janssen, MSD, and Eli Lilly. HMO reports grant/research support from Janssen and Novartis; is a consultant for AbbVie, Celgene, Janssen, Eli Lilly, Novartis, Pfizer, and UCB; and received speakers’ bureau fees from AbbVie, Celgene, Janssen, Lilly, Novartis, Pfizer, and UCB. LSG reports grant/research support from UCB, AbbVie, Amgen, Novartis, and Pfizer and consulting fees from Galapagos, Eli Lilly, Janssen, Novartis, Pfizer, and UCB. FVDB reports research grants, consultancy fees, or speaker honoraria from AbbVie, BMS, Celgene, Galapagos, Janssen, Eli Lilly, Merck, Novartis, Pfizer, and UCB. SH reports consulting or speaking fees from Novartis, Merck, Janssen, Pfizer, Eli Lilly, and UCB and research grants from AbbVie, UCB, Janssen, and Merck. HK reports grant/research support from AbbVie, Asahi-Kasei, Chugai, Eisai, Mitsubishi-Tanabe, and Novartis; consulting fees from AbbVie, Boehringer, Celgene, Eli Lilly, Janssen, Novartis, Sanofi, and UCB; and received speakers’ bureau fees from AbbVie, Asahi-Kasei, BMS, Chugai, Eisai, Eli Lilly, Janssen, Mitsubishi-Tanabe, Novartis, and Pfizer. DP reports research grants from AbbVie, Eli Lilly, MSD, Novartis, and Pfizer; consultation fees from AbbVie, BMS, Eli Lilly, MSD, Novartis, Pfizer, UCB, and Celgene; and speaker fees from AbbVie, BMS, Eli Lilly, MSD, Novartis, Pfizer, UCB, and Roche. MVDS reports grant/research support from Novartis, Eli Lilly, Boehringer Ingelheim, Janssen, and UCB; consultant fees from AbbVie, Novartis, Eli Lily, and MSD; and speaker fees from Novartis and MSD. ASW, BOP, AS, HBS, and SH are employees of Novartis and own Novartis stock. AD reports receiving honoraria for consulting or speaking for or research grants from AbbVie, Amgen, Boehringer Ingelheim, Celgene, Eli Lilly, Galapagos, GSK, Janssen, Novartis, Pfizer, and UCB.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
