

Temporal trends in emergency admissions for diabetic ketoacidosis in people with diabetes in England before and during the COVID-19 pandemic: a population-based study
- PMID: 34481558
- PMCID: PMC9765220
- DOI: 10.1016/S2213-8587(21)00208-4
Temporal trends in emergency admissions for diabetic ketoacidosis in people with diabetes in England before and during the COVID-19 pandemic: a population-based study
Abstract
Background: Diabetic ketoacidosis (DKA) has been reported to be increasing in frequency during the COVID-19 pandemic. We aimed to examine the rates of DKA hospital admissions and the patient demographics associated with DKA during the pandemic compared with in prepandemic years.
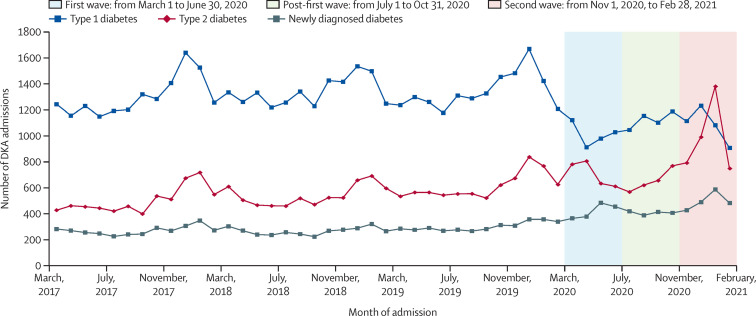
Methods: Using a comprehensive, multiethnic, national dataset, the Secondary Uses Service repository, we extracted all emergency hospital admissions in England coded with DKA from March 1 to June 30, 2020 (first wave of the pandemic), July 1 to Oct 31, 2020 (post-first wave), and Nov 1, 2020, to Feb 28, 2021 (second wave), and compared these with DKA admissions in the equivalent periods in 2017-20. We also examined baseline characteristics, mortality, and trends in patients who were admitted with DKA.
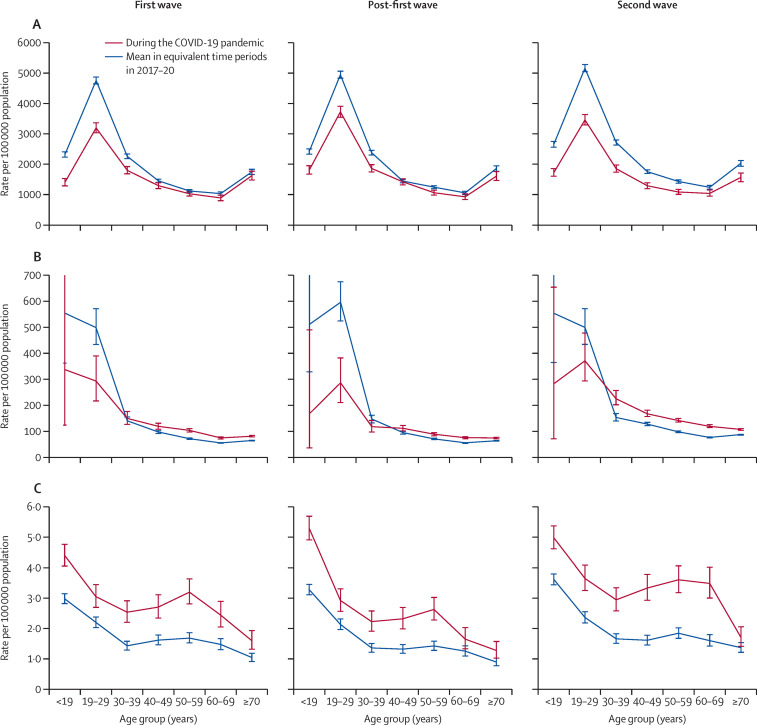
Findings: There were 8553 admissions coded with DKA during the first wave, 8729 during the post-first wave, and 10 235 during the second wave. Compared with preceding years, DKA admissions were 6% (95% CI 4-9; p<0·0001) higher in the first wave of the pandemic (from n=8048), 6% (3-8; p<0·0001) higher in the post-first wave (from n=8260), and 7% (4-9; p<0·0001) higher in the second wave (from n=9610). In the first wave, DKA admissions reduced by 19% (95% CI 16-21) in those with pre-existing type 1 diabetes (from n=4965 to n=4041), increased by 41% (35-47) in those with pre-existing type 2 diabetes (from n=2010 to n=2831), and increased by 57% (48-66) in those with newly diagnosed diabetes (from n=1072 to n=1681). Compared with prepandemic, type 2 diabetes DKA admissions were similarly common in older individuals and men but were higher in those of non-White ethnicities during the first wave. The increase in newly diagnosed DKA admissions occurred across all age groups and these were significantly increased in men and people of non-White ethnicities. In the post-first wave, DKA admissions did not return to the baseline level of previous years; DKA admissions were 14% (11-17) lower in patients with type 1 diabetes (from n=5208 prepandemic to n=4491), 30% (24-36) higher in patients with type 2 diabetes (from n=2011 to n=2613), and 56% (47-66) higher in patients with newly diagnosed diabetes (from n=1041 to n=1625). During the second wave, DKA admissions were 25% (22-27) lower in patients with type 1 diabetes (from n=5769 prepandemic to n=4337), 50% (44-56) higher in patients with type 2 diabetes (from n=2608 to n=3912), and 61% (52-70) higher in patients with newly diagnosed diabetes (from n=1234 to n=1986).
Interpretation: Our results provide evidence for differences in the numbers and characteristics of people presenting with DKA during the COVID-19 pandemic compared with in the preceding 3 years. Greater awareness of risk factors for DKA in type 2 diabetes and vigilance for newly diagnosed diabetes presenting with DKA during the COVID-19 pandemic might help mitigate the increased impact of DKA.
Funding: None.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests SM, EB, PK, BY, KK, and JV are members of clinical advisory groups to the NDA. SM is a trustee of the Diabetes Research and Wellness Foundation and has a grant in support of an investigator-initiated study from DexCom. PK, BY, KK, and JV are members of the NDA research committee. ST has received honoraria for speaking from Lilly and Sanofi-Aventis. KD has received honoraria for speaking and travel grants from Novo Nordisk, Sanofi-Aventis, Lilly, and Boehringer Ingelheim, and consulting fees from Sanofi-Aventis; is Chair of the Joint British Diabetes Societies for Inpatient Care; and is committee member of the Association of British Clinical Diabetologists. PK is National Specialty Adviser for Diabetes and Obesity at NHS England and NHS Improvement. BY is clinical lead for the NDA and a trustee of Diabetes UK. KK has been a consultant and speaker for Novartis, Novo Nordisk, Sanofi-Aventis, Lilly, and Merck Sharp & Dohme; has received grants in support of investigator-initiated studies from Novartis, Novo Nordisk, Sanofi-Aventis, Lilly, Merck Sharp & Dohme, Pfizer, and Boehringer Ingelheim; has served on advisory boards for Novo Nordisk, Sanofi-Aventis, Lilly, and Merck Sharp & Dohme; and is Chair of the Ethnicity Subgroup of Scientific Advisory Group for Emergencies (SAGE) and member of SAGE. JV is the National Clinical Director for Diabetes and Obesity at NHS England and NHS Improvement. EV declares no competing interests.
Figures
Comment in
-
Diabetic ketoacidosis risk during the COVID-19 pandemic.Lancet Diabetes Endocrinol. 2021 Oct;9(10):643-644. doi: 10.1016/S2213-8587(21)00241-2. Epub 2021 Sep 2. Lancet Diabetes Endocrinol. 2021. PMID: 34481553 Free PMC article. No abstract available.
References
-
- Dhatariya K. Glaser, Codner E, Umpierrez GE. Diabetic ketoacidosis. Nat Rev Dis Primers. 2020;6:41. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
