

Brain stimulation treatments in epilepsy: Basic mechanisms and clinical advances
- PMID: 34482013
- PMCID: PMC9133258
- DOI: 10.1016/j.bj.2021.08.010
Brain stimulation treatments in epilepsy: Basic mechanisms and clinical advances
Abstract
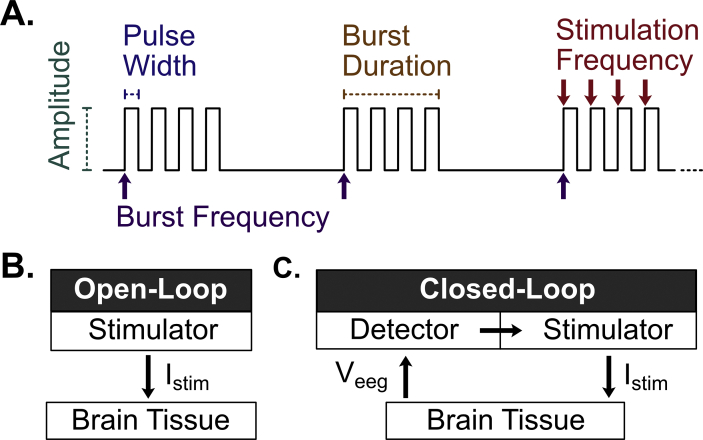
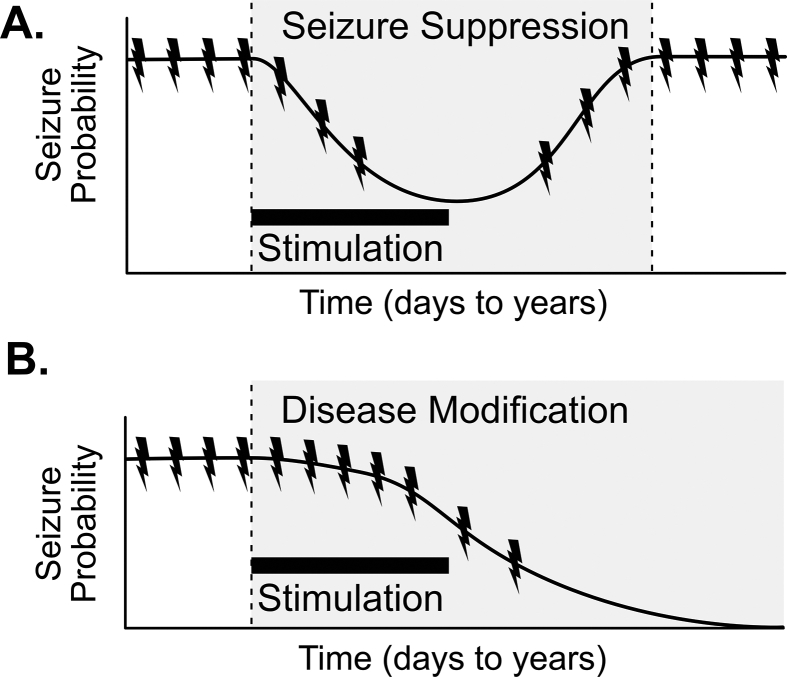
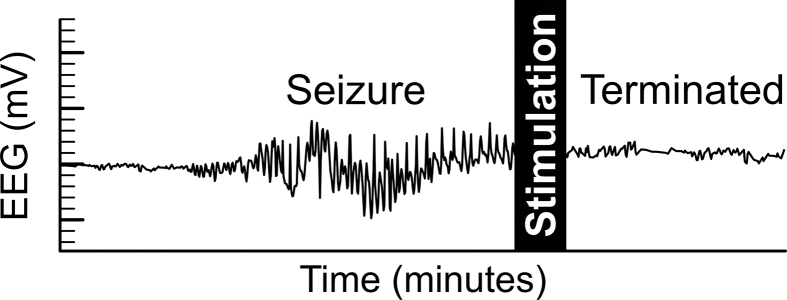
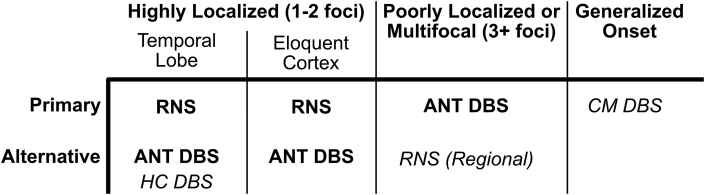
Drug-resistant epilepsy, characterized by ongoing seizures despite appropriate trials of anti-seizure medications, affects approximately one-third of people with epilepsy. Brain stimulation has recently become available as an alternative treatment option to reduce symptomatic seizures in short and long-term follow-up studies. Several questions remain on how to optimally develop patient-specific treatments and manage therapy over the long term. This review aims to discuss the clinical use and mechanisms of action of Responsive Neural Stimulation and Deep Brain Stimulation in the treatment of epilepsy and highlight recent advances that may both improve outcomes and present new challenges. Finally, a rational approach to device selection is presented based on current mechanistic understanding, clinical evidence, and device features.
Keywords: Deep brain stimulation; Epilepsy; Neurostimulation; Responsive neural stimulation; Seizure.
Copyright © 2021 Chang Gung University. Published by Elsevier B.V. All rights reserved.
Figures
References
-
- Abdel-Mannan O., Sutcliffe A.G. A national surveillance study of childhood epilepsy mortality in the UK and Ireland. Eur J Neurol. 2020;27:327–333. - PubMed
-
- Perucca P., Gilliam F.G. Adverse effects of antiepileptic drugs. Lancet Neurol. 2012;11:792–802. Erratum in: Lancet Neurol 2012;11:746. - PubMed
-
- Kwan P., Brodie M.J. Early identification of refractory epilepsy. N Engl J Med. 2000;342:314–319. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
