

Ex vivo lung perfusion: how we do it
- PMID: 34483507
- PMCID: PMC8408366
- DOI: 10.1007/s12055-021-01215-z
Ex vivo lung perfusion: how we do it
Abstract
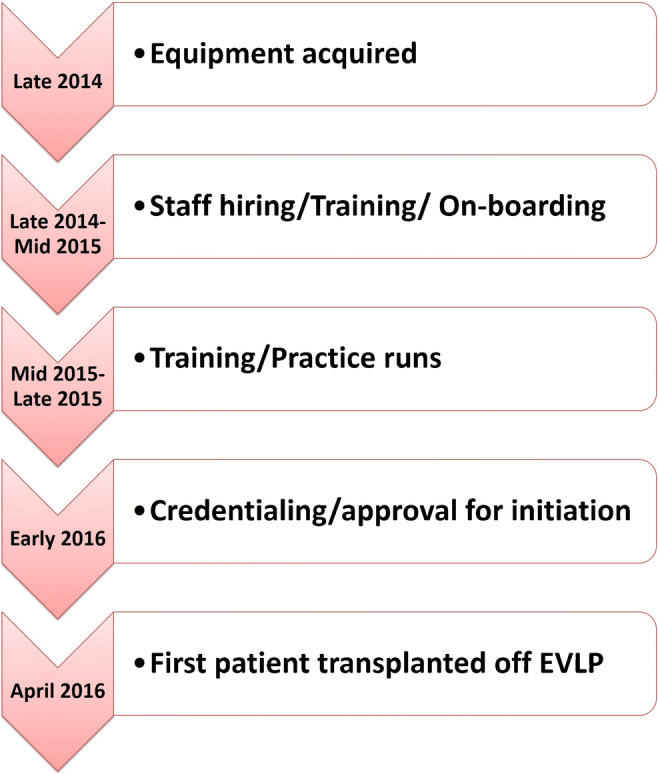
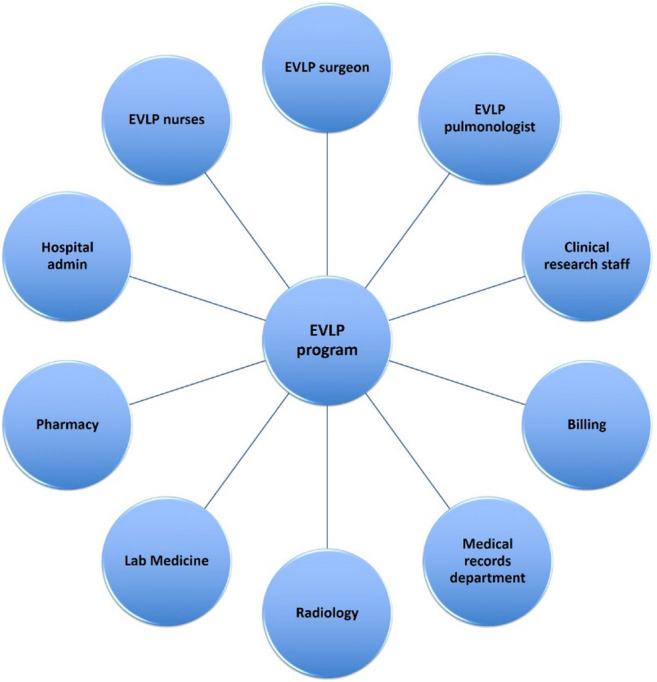
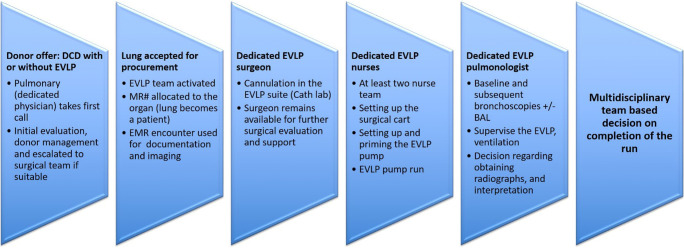
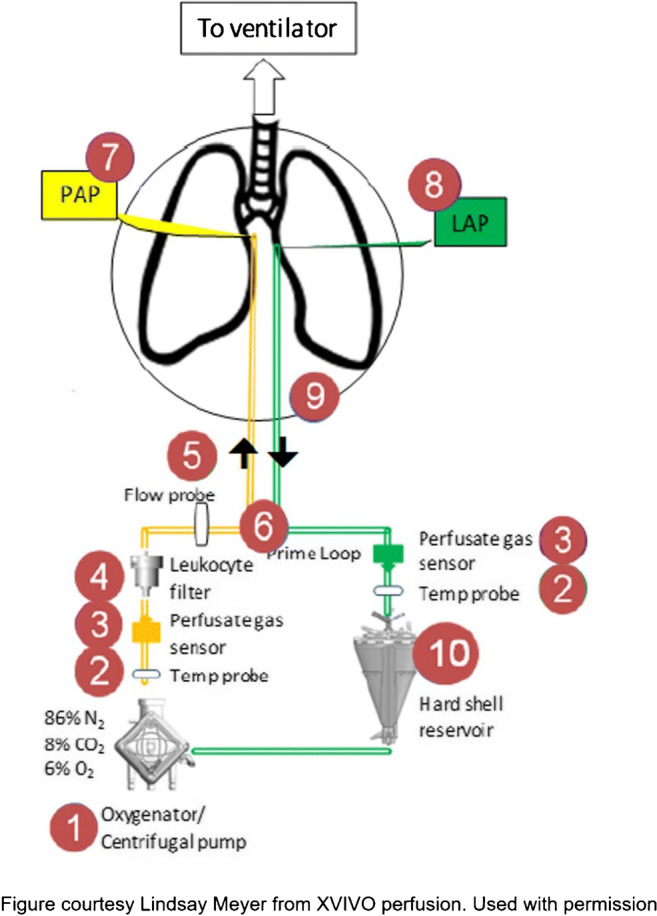
Lung transplantation is an established treatment for patients with end-stage lung disease. However, a shortage of donors, low lung utilization among potential donors, and waitlist mortality continue to be challenges. In the last decade, ex vivo lung perfusion (EVLP) has expanded the donor pool by allowing prolonged evaluation of marginal donor lungs and allowing reparative therapies for lungs, which are otherwise considered not transplantable. In this review, we describe in detail our experience with EVLP including our workflow, setup, operative technique, and protocols. Our multidisciplinary EVLP program functions with the collaboration of surgeons, pulmonologists, and EVLP nurses who run the pump. EVLP program has been a valuable addition to our program. Since Food and Drug Administration (FDA) approval in 2019, we experienced incremental increased lung transplant volume of 12% annually.
Keywords: Donor selection; Ex vivo lung perfusion; Lung transplantation.
© The Author(s) 2021.
Conflict of interest statement
Conflict of interestThe authors declare no competing interests.
Figures

References
-
- Organ Procurement and Transplantation Network (OPTN). Data as of Dec 31, 2020. Available at https://optn.transplant.hrsa.gov. Accessed 1 Feb 2021
-
- Charles EJ, Huerter ME, Wagner CE, Sharma AK, Zhao Y, Stoler MH, Mehaffey JH, Isbell JM, Lau CL, Tribble CG, Laubach VE, Kron IL. Donation after circulatory death lungs transplantable up to six hours after ex vivo lung perfusion. Ann Thorac Surg. 2016;102:1845–1853. doi: 10.1016/j.athoracsur.2016.06.043. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources