

Clinical Benefits and Safety of Gemtuzumab Ozogamicin in Treating Acute Myeloid Leukemia in Various Subgroups: An Updated Systematic Review, Meta-Analysis, and Network Meta-Analysis
- PMID: 34484181
- PMCID: PMC8415423
- DOI: 10.3389/fimmu.2021.683595
Clinical Benefits and Safety of Gemtuzumab Ozogamicin in Treating Acute Myeloid Leukemia in Various Subgroups: An Updated Systematic Review, Meta-Analysis, and Network Meta-Analysis
Abstract
Background: Previous trials demonstrated evidence involving the total effects of gemtuzumab ozogamicin (GO), an anti-CD33 humanized antibody, on treating acute myeloid leukemia (AML). In this updated systematic review, meta-analysis, and network meta-analysis (NMA), we aimed to comprehensively explore the clinical benefits and safety of GO in various subtypes of AML.
Methods: PubMed, Embase, Cochrane, and Chinese databases were filtered to search randomized controlled trials (RCTs) and retrospective cohort studies that compared clinical efficiency and toxicity of GO with non-GO groups in AML. Random-effects models were used to calculate pooled effect sizes and 95% confidence intervals (CIs). Relative risk (RR) was used for estimating complete remission (CR), early death, and toxicity. Hazard risk (HR) was accomplished to evaluate survival.
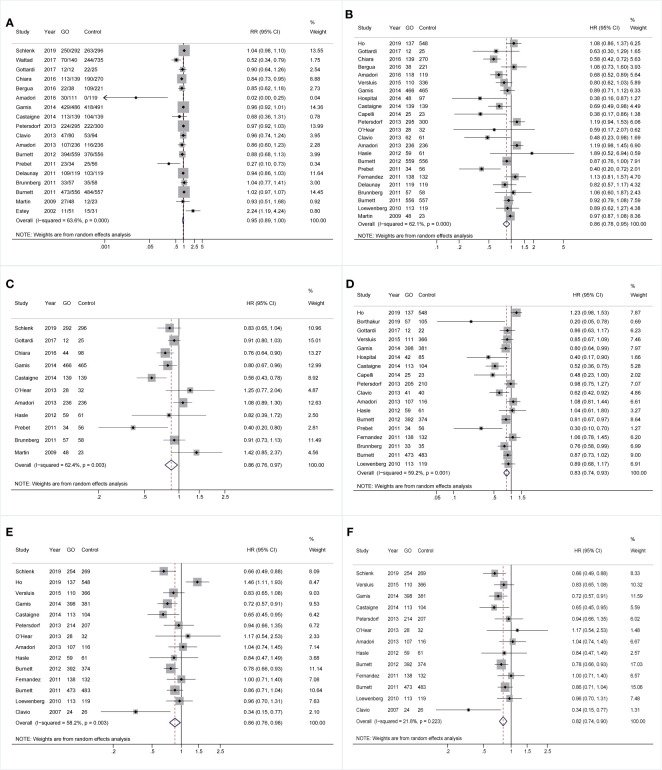
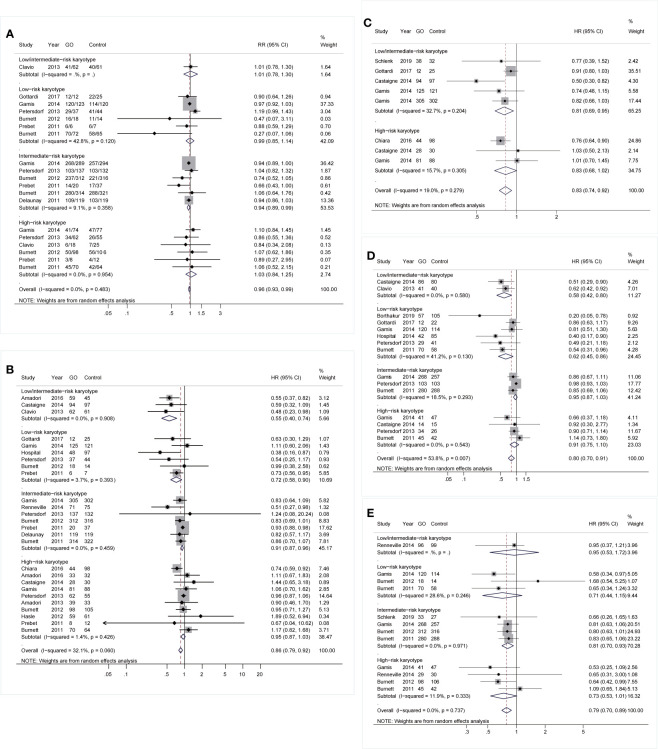
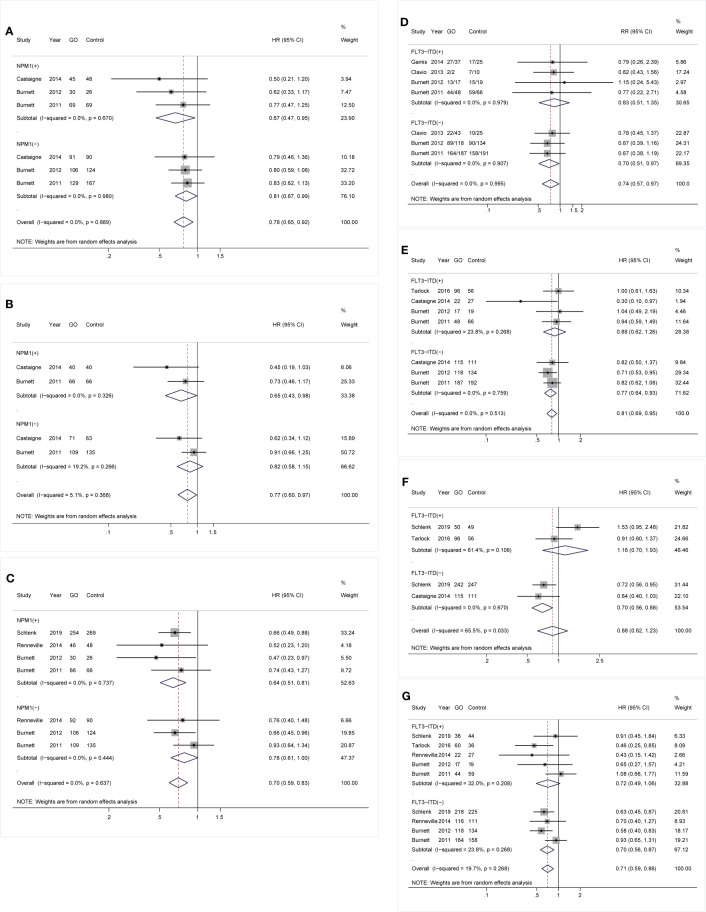
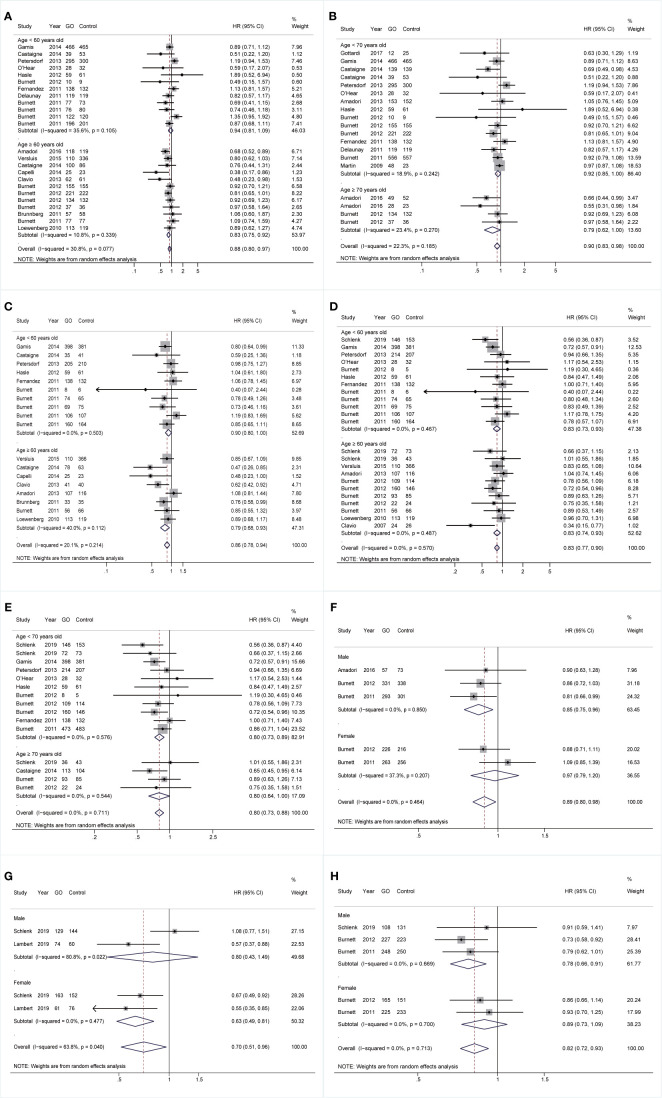
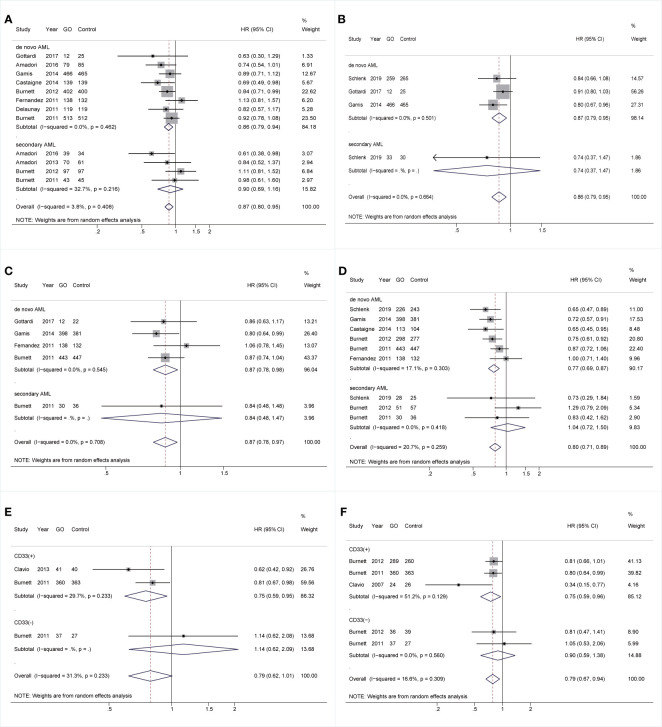
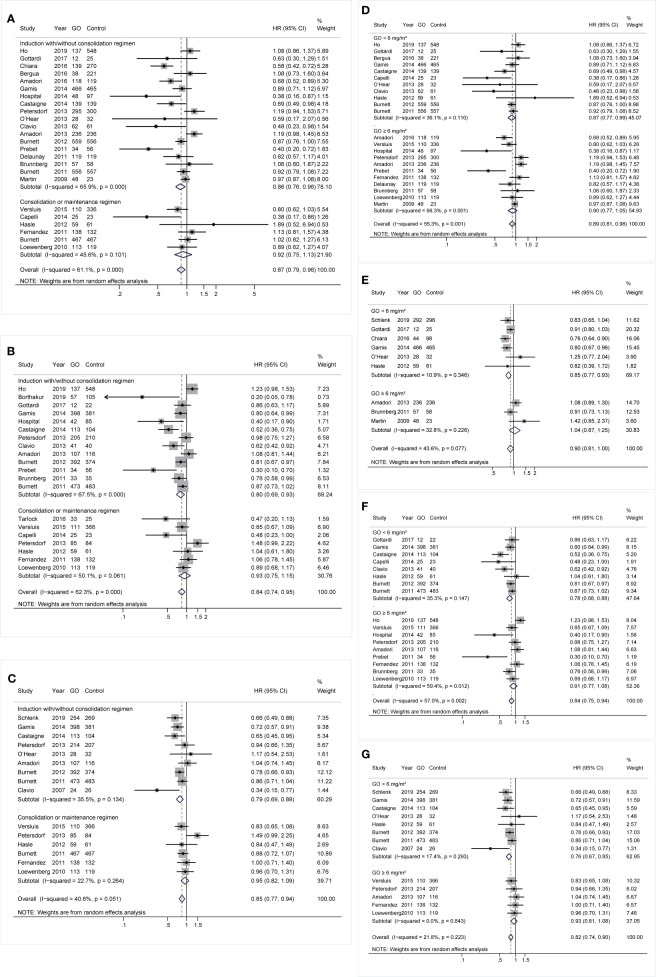
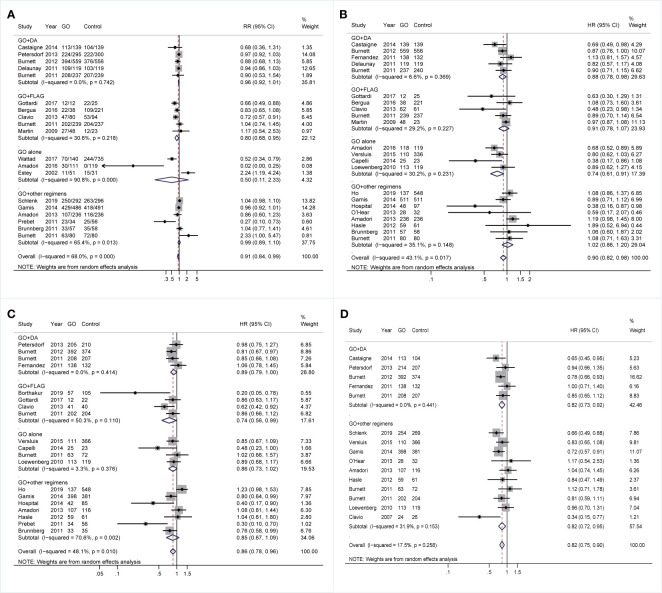
Results: Fifteen RCTs and 15 retrospective cohort studies were identified (GO: 4,768; Control: 6,466). GO tended to improve CR (RR 0.95, p = 0.084), followed by significantly improved survival (overall survival: HR 0.86, p = 0.003; event-free survival: HR 0.86, p = 0.015; relapse-free survival: HR 0.83, p = 0.001; cumulative incidence of relapse: HR 0.82, p < 0.001). GO benefits of CR and survival were evident in favorable- and intermediate-risk karyotypes (p ≤ 0.023). GO advantages were also associated with nucleophosmin 1 mutations (p ≤ 0.04), wild-type FMS-like tyrosine kinase 3 internal tandem duplication gene (p ≤ 0.03), age of <70 years (p < 0.05), de novo AML (p ≤ 0.017), and CD33(+) (p ≤ 0.021). Both adding GO into induction therapy (p ≤ 0.011) and a lower (<6 mg/m2) dose of GO (p ≤ 0.03) enhanced survival. Prognosis of combined regimens with GO was heterogeneous in both meta-analysis and NMA, with several binding strategies showing improved prognosis. Additionally, GO was related to increased risk of early death at a higher dose (≥6 mg/m2) (RR 2.01, p = 0.005), hepatic-related adverse effects (RR 1.29, p = 0.02), and a tendency of higher risk for hepatic veno-occlusive disease or sinusoidal obstruction syndrome (RR 1.56, p = 0.072).
Conclusions: These data indicated therapeutic benefits and safety of GO in AML, especially in some subtypes, for which further head-to-head RCTs are warranted.
Systematic review registration: [PROSPERO: https://www.crd.york.ac.uk/prospero/], identifier [CRD42020158540].
Keywords: acute myeloid leukemia; gemtuzumab ozogamicin; meta-analysis; network meta-analysis; response; survival; toxicity.
Copyright © 2021 Xu, He and Yu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Efficacy and safety of adding gemtuzumab ozogamicin to conventional chemotherapy for adult acute myeloid leukemia: a systematic review and meta-analysis.Hematology. 2022 Dec;27(1):53-64. doi: 10.1080/16078454.2021.2013410. Hematology. 2022. PMID: 34957930
-
Gemtuzumab Ozogamicin Improves Event-Free Survival and Reduces Relapse in Pediatric KMT2A-Rearranged AML: Results From the Phase III Children's Oncology Group Trial AAML0531.J Clin Oncol. 2021 Oct 1;39(28):3149-3160. doi: 10.1200/JCO.20.03048. Epub 2021 May 28. J Clin Oncol. 2021. PMID: 34048275 Free PMC article. Clinical Trial.
-
Gemtuzumab ozogamicin for treatment of newly diagnosed CD33-positive acute myeloid leukemia.Future Oncol. 2018 Dec;14(30):3199-3213. doi: 10.2217/fon-2018-0325. Epub 2018 Jul 24. Future Oncol. 2018. PMID: 30039981 Free PMC article.
-
Effect of adding gemtuzumab ozogamicin to induction chemotherapy for newly diagnosed acute myeloid leukemia: a meta-analysis of prospective randomized phase III trials.Ann Oncol. 2014 Feb;25(2):455-61. doi: 10.1093/annonc/mdt566. Ann Oncol. 2014. PMID: 24478322
-
ABCB1 SNP predicts outcome in patients with acute myeloid leukemia treated with Gemtuzumab ozogamicin: a report from Children's Oncology Group AAML0531 Trial.Blood Cancer J. 2019 May 21;9(6):51. doi: 10.1038/s41408-019-0211-y. Blood Cancer J. 2019. PMID: 31113932 Free PMC article. Clinical Trial.
Cited by
-
Older Patients with Acute Myeloid Leukemia Deserve Individualized Treatment.Curr Oncol Rep. 2022 Nov;24(11):1387-1400. doi: 10.1007/s11912-022-01299-9. Epub 2022 Jun 2. Curr Oncol Rep. 2022. PMID: 35653050 Free PMC article. Review.
-
A ten-gene DNA-damage response pathway gene expression signature predicts gemtuzumab ozogamicin response in pediatric AML patients treated on COGAAML0531 and AAML03P1 trials.Leukemia. 2022 Aug;36(8):2022-2031. doi: 10.1038/s41375-022-01622-0. Epub 2022 Jun 10. Leukemia. 2022. PMID: 35688939 Free PMC article.
-
Monoclonal Antibodies Against Myeloid Leukemia Cells: Current Knowledge and Future Directions.Int J Mol Sci. 2025 May 10;26(10):4571. doi: 10.3390/ijms26104571. Int J Mol Sci. 2025. PMID: 40429716 Free PMC article. Review.
-
Gemtuzumab ozogamicin for relapsed or primary refractory acute myeloid leukemia in children-the Polish Pediatric Leukemia and Lymphoma Study Group experience.Front Immunol. 2023 Dec 22;14:1268993. doi: 10.3389/fimmu.2023.1268993. eCollection 2023. Front Immunol. 2023. PMID: 38187390 Free PMC article.
-
The Immune Resistance Signature of Acute Myeloid Leukemia and Current Immunotherapy Strategies.Cancers (Basel). 2024 Jul 23;16(15):2615. doi: 10.3390/cancers16152615. Cancers (Basel). 2024. PMID: 39123343 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous