

COVID-19 and Acute Coronary Syndromes: From Pathophysiology to Clinical Perspectives
- PMID: 34484561
- PMCID: PMC8410438
- DOI: 10.1155/2021/4936571
COVID-19 and Acute Coronary Syndromes: From Pathophysiology to Clinical Perspectives
Abstract
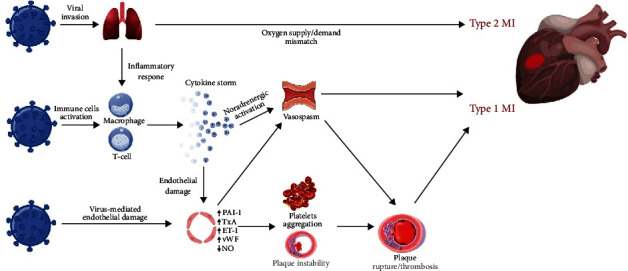
Acute coronary syndromes (ACS) are frequently reported in patients with coronavirus disease 2019 (COVID-19) and may impact patient clinical course and mortality. Although the underlying pathogenesis remains unclear, several potential mechanisms have been hypothesized, including oxygen supply/demand imbalance, direct viral cellular damage, systemic inflammatory response with cytokine-mediated injury, microvascular thrombosis, and endothelial dysfunction. The severe hypoxic state, combined with other conditions frequently reported in COVID-19, namely sepsis, tachyarrhythmias, anemia, hypotension, and shock, can induce a myocardial damage due to the mismatch between oxygen supply and demand and results in type 2 myocardial infarction (MI). In addition, COVID-19 promotes atherosclerotic plaque instability and thrombus formation and may precipitate type 1 MI. Patients with severe disease often show decrease in platelets count, higher levels of d-dimer, ultralarge von Willebrand factor multimers, tissue factor, and prolongation of prothrombin time, which reflects a prothrombotic state. An endothelial dysfunction has been described as a consequence of the direct viral effects and of the hyperinflammatory environment. The expression of tissue factor, von Willebrand factor, thromboxane, and plasminogen activator inhibitor-1 promotes the prothrombotic status. In addition, endothelial cells generate superoxide anions, with enhanced local oxidative stress, and endothelin-1, which affects the vasodilator/vasoconstrictor balance and platelet aggregation. The optimal management of COVID-19 patients is a challenge both for logistic and clinical reasons. A deeper understanding of ACS pathophysiology may yield novel research insights and therapeutic perspectives in higher cardiovascular risk subjects with COVID-19.
Copyright © 2021 Luca Esposito et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest. The authors have no commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
