

Coronary Magnetic Resonance Angiography in Chronic Coronary Syndromes
- PMID: 34485397
- PMCID: PMC8416045
- DOI: 10.3389/fcvm.2021.682924
Coronary Magnetic Resonance Angiography in Chronic Coronary Syndromes
Abstract
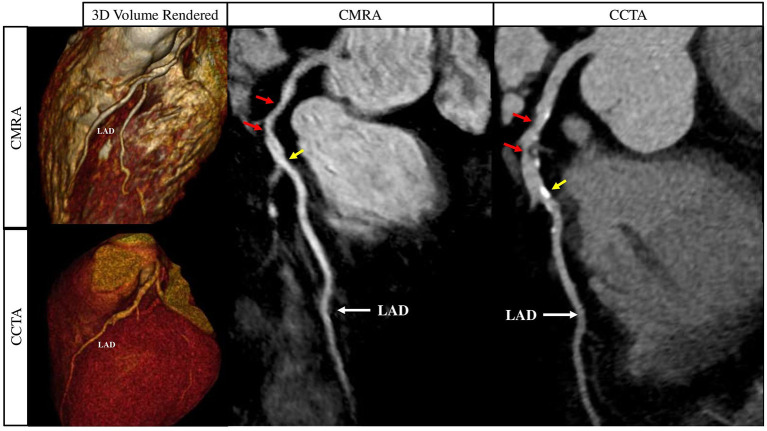
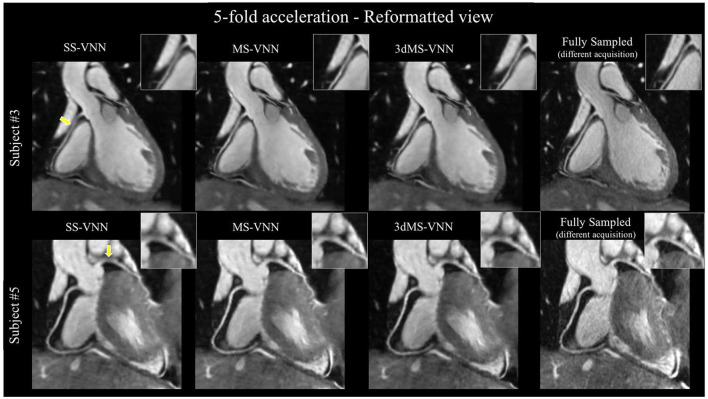
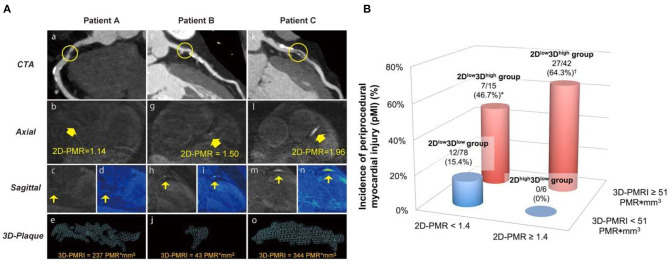
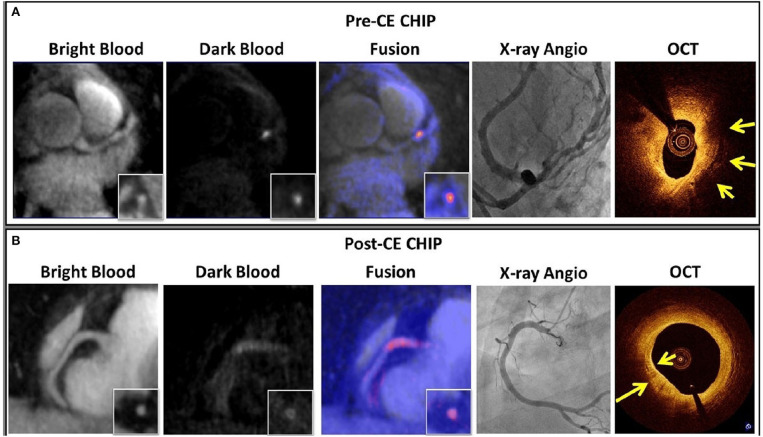
Cardiovascular disease is the leading cause of mortality worldwide, with atherosclerotic coronary artery disease (CAD) accounting for the majority of cases. X-ray coronary angiography and computed tomography coronary angiography (CCTA) are the imaging modalities of choice for the assessment of CAD. However, the use of ionising radiation and iodinated contrast agents remain drawbacks. There is therefore a clinical need for an alternative modality for the early identification and longitudinal monitoring of CAD without these associated drawbacks. Coronary magnetic resonance angiography (CMRA) could be a potential alternative for the detection and monitoring of coronary arterial stenosis, without exposing patients to ionising radiation or iodinated contrast agents. Further advantages include its versatility, excellent soft tissue characterisation and suitability for repeat imaging. Despite the early promise of CMRA, widespread clinical utilisation remains limited due to long and unpredictable scan times, onerous scan planning, lower spatial resolution, as well as motion related image quality degradation. The past decade has brought about a resurgence in CMRA technology, with significant leaps in image acceleration, respiratory and cardiac motion estimation and advanced motion corrected or motion-resolved image reconstruction. With the advent of artificial intelligence, great advances are also seen in deep learning-based motion estimation, undersampled and super-resolution reconstruction promising further improvements of CMRA. This has enabled high spatial resolution (1 mm isotropic), 3D whole heart CMRA in a clinically feasible and reliable acquisition time of under 10 min. Furthermore, latest super-resolution image reconstruction approaches which are currently under evaluation promise acquisitions as short as 1 min. In this review, we will explore the recent technological advances that are designed to bring CMRA closer to clinical reality.
Keywords: CCS; CMRA; atherosclerosis; coronary angiography; magnetic resonance imaging; plaque.
Copyright © 2021 Hajhosseiny, Munoz, Cruz, Khamis, Kim, Prieto and Botnar.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
-
- Institute for Health Metrics and Evaluation (IHME) . GBD Compare. Available online at: https://vizhub.healthdata.org/gbd-compare/ (accessed June 6, 2021).
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous