

Viral Coinfection among COVID-19 Patient Groups: An Update Systematic Review and Meta-Analysis
- PMID: 34485513
- PMCID: PMC8416381
- DOI: 10.1155/2021/5313832
Viral Coinfection among COVID-19 Patient Groups: An Update Systematic Review and Meta-Analysis
Abstract
Background: Coinfections have a potential role in increased morbidity and mortality rates during pandemics. Our investigation is aimed at evaluating the viral coinfection prevalence in COVID-19 patients.
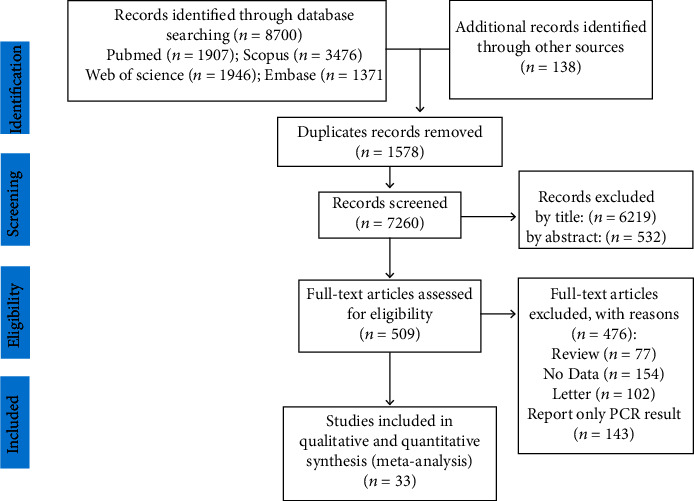
Methods: We systematically searched scientific databases, including Medline, Scopus, WOS, and Embase, from December 1, 2019, to December 30, 2020. Preprint servers such as medRxiv were also scanned to find other related preprint papers. All types of studies evaluating the viral coinfection prevalence in COVID-19 patients were considered. We applied the random effects model to pool all of the related studies.
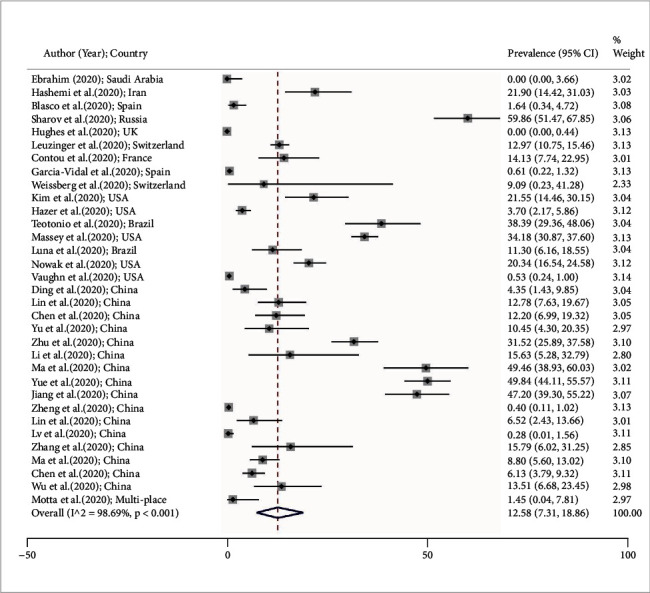
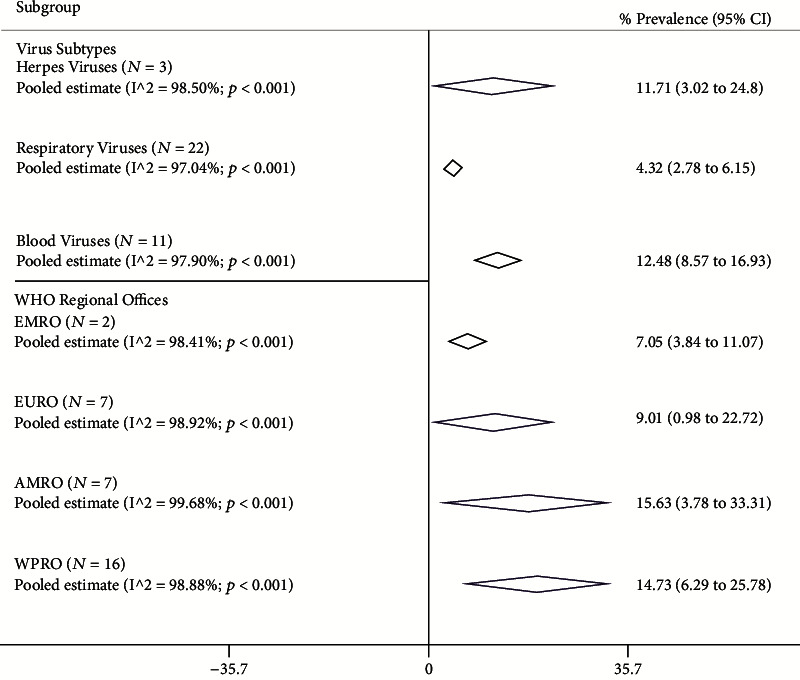
Results: Thirty-three studies including 10484 patients were identified. The viral coinfection estimated pooled prevalence was 12.58%; 95% CI: 7.31 to 18.96). Blood viruses (pooled prevalence: 12.48%; 95% CI: 8.57 to 16.93) had the most frequent viral coinfection, and respiratory viruses (pooled prevalence: 4.32%; 95% CI: 2.78 to 6.15) had less frequent viral coinfection. The herpesvirus pooled prevalence was 11.71% (95% CI: 3.02 to 24.80). Also, the maximum and minimum of viral coinfection pooled prevalence were in AMRO and EMRO with 15.63% (95% CI: 3.78 to 33.31) and 7.05% (95% CI: 3.84 to 11.07), respectively.
Conclusion: The lowest rate of coinfection belonged to respiratory viruses. Blood-borne viruses had the highest coinfection rate. Our results provide important data about the prevalence of blood-borne viruses among COVID-19 patients which can be critical when it comes to their treatment procedure.
Copyright © 2021 Pooneh Malekifar et al.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
References
-
- Organization WH. Weekly epidemiological update—2 February 2021. World Health Organization; 2021.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
