

Improved collection of hematopoietic stem cells and progenitors from Fanconi anemia patients for gene therapy purposes
- PMID: 34485595
- PMCID: PMC8390450
- DOI: 10.1016/j.omtm.2021.06.001
Improved collection of hematopoietic stem cells and progenitors from Fanconi anemia patients for gene therapy purposes
Abstract
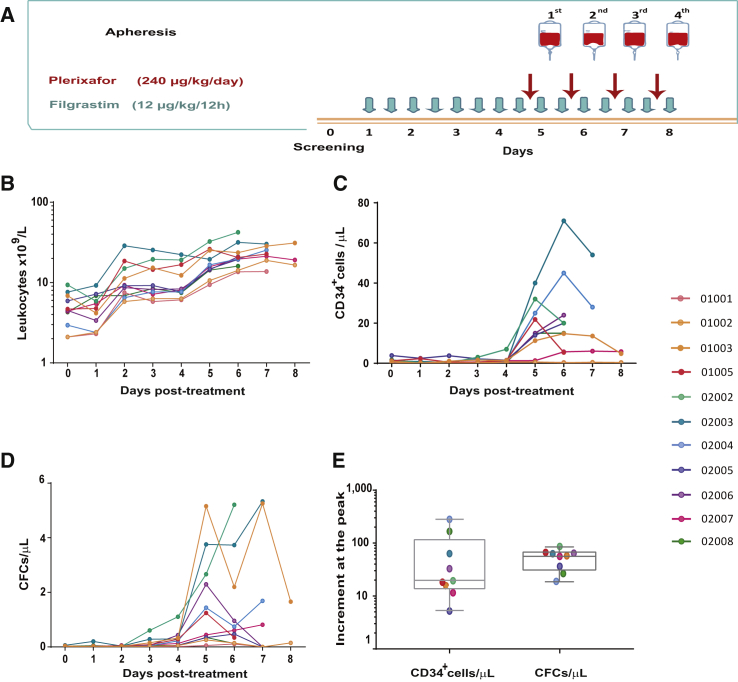
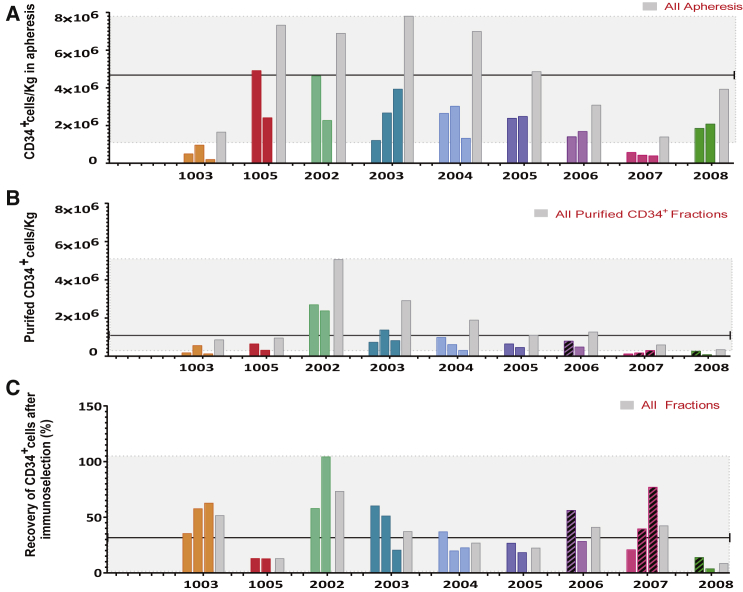
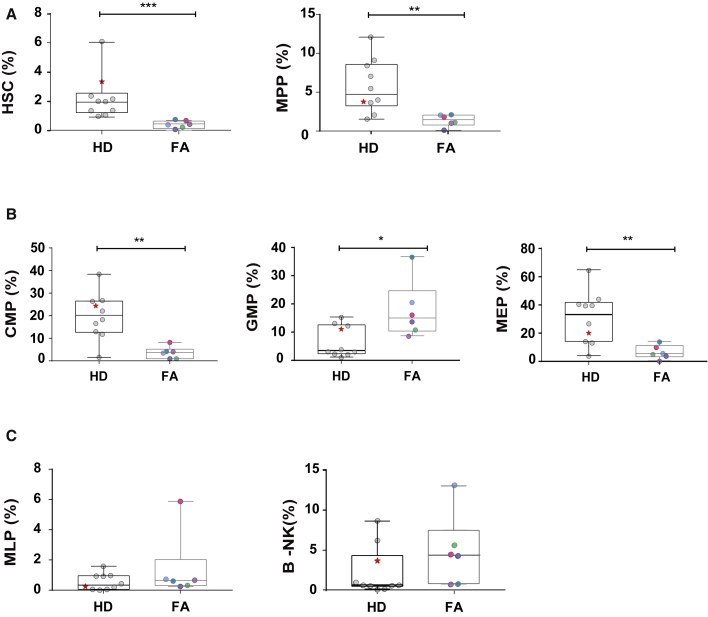
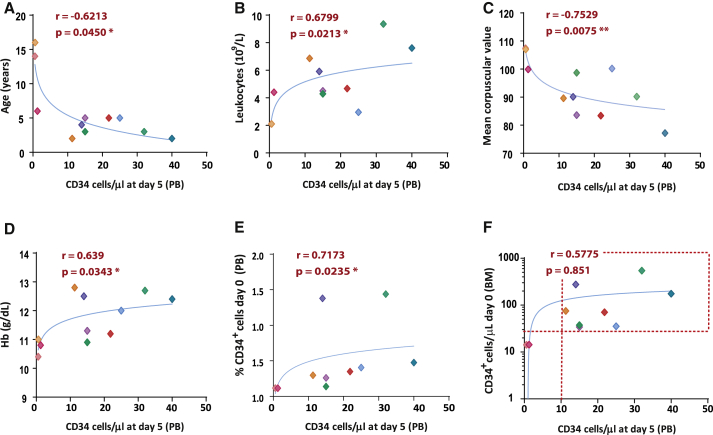
Difficulties in the collection of hematopoietic stem and progenitor cells (HSPCs) from Fanconi anemia (FA) patients have limited the gene therapy in this disease. We have investigated (ClinicalTrials.gov, NCT02931071) the safety and efficacy of filgrastim and plerixafor for mobilization of HSPCs and collection by leukapheresis in FA patients. Nine of eleven enrolled patients mobilized beyond the threshold level of 5 CD34+ cells/μL required to initiate apheresis. A median of 21.8 CD34+ cells/μL was reached at the peak of mobilization. Significantly, the oldest patients (15 and 16 years old) were the only ones who did not reach that threshold. A median of 4.27 million CD34+ cells/kg was collected in 2 or 3 aphereses. These numbers were markedly decreased to 1.1 million CD34+ cells/kg after immunoselection, probably because of weak expression of the CD34 antigen. However, these numbers were sufficient to facilitate the engraftment of corrected HSPCs in non-conditioned patients. No procedure-associated serious adverse events were observed. Mobilization of CD34+ cells correlated with younger age, higher leukocyte counts and hemoglobin values, lower mean corpuscular volume, and higher proportion of CD34+ cells in bone marrow (BM). All these values offer crucial information for the enrollment of FA patients for gene therapy protocols.
Keywords: AMD3100; Fanconi anemia; HSPC collection; Mozobil; filgrastim; gene therapy; lentiviral vector; leukapheresis; mobilization; plerixafor.
© 2021 The Author(s).
Conflict of interest statement
J. Sevilla is a consultant and advisor and has received honorarium (Amgen, Novartis, Miltenyi, Sobi, Rocket Pharmaceuticals Inc.) and has licensed medicinal products from Rocket Pharmaceuticals Inc. S.N. and P.R. have licensed medicinal products and receive research funding and equity from Rocket Pharmaceuticals Inc. J.C.S.: Rocket Pharmaceuticals Inc.: consultant/incomes from licensed medicinal products/research funding/equity. J. Schwartz is Medical Director of Rocket Pharmaceuticals Inc. J. Surralles: service agreements (Rocket Pharmaceuticals Inc.). J.A.B.: Rocket Pharmaceuticals Inc.: consultant/incomes from licensed medicinal products/research funding/equity; Roche: honorarium; Pfizer: honorarium.
Figures
References
-
- Naldini L. Ex vivo gene transfer and correction for cell-based therapies. Nat. Rev. Genet. 2011;12:301–315. - PubMed
-
- Tisdale J.F., Pierciey F.J., Jr., Bonner M., Thompson A.A., Krishnamurti L., Mapara M.Y., Kwiatkowski J.L., Shestopalov I., Ribeil J.A., Huang W. Safety and feasibility of hematopoietic progenitor stem cell collection by mobilization with plerixafor followed by apheresis vs bone marrow harvest in patients with sickle cell disease in the multi-center HGB-206 trial. Am. J. Hematol. 2020;95:E239–E242. - PubMed
-
- Wong J.C., Alon N., Norga K., Kruyt F.A., Youssoufian H., Buchwald M. Cloning and analysis of the mouse Fanconi anemia group A cDNA and an overlapping penta zinc finger cDNA. Genomics. 2000;67:273–283. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
